Zhou Xuan, Ma Tingting, Zhang Yichan, Zhou Na, Li Juan
Department of Hematology, The Affiliated Drum Tower Hospital of Nanjing University Medical School, Gulou District, Nanjing, China.
PLoS One. 2017 Mar 29;12(3):e0174648. doi: 10.1371/journal.pone.0174648. eCollection 2017.
The addition of rituximab to standard chemotherapy has significantly improved survival in patients with lymphoma. Recently, maintenance therapy with rituximab has been shown to prevent relapse and provide survival benefits for patients with follicular or mantle cell lymphoma. However, the effects of rituximab in patients with diffuse large B-cell lymphoma (DLBCL) remain unclear. Two new studies involving rituximab in the treatment of DLBCL were performed this past year. We performed a meta analysis to evaluate the effects of rituximab maintenance treatment of patients with DLBCL.
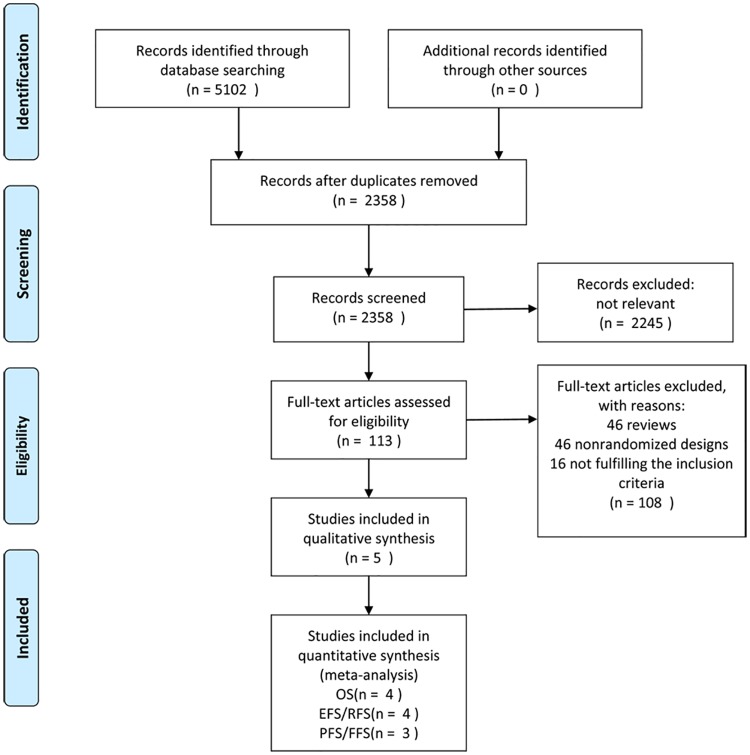
Several databases (PubMed, MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials) databases were reviewed for relevant randomized controlled trials published prior to May, 2016. Two reviewers assessed the quality of the included studies and extracted data independently. The hazard ratios (HRs) for time-to-event data and relative risks (RRs) for the other data were pooled and estimated.
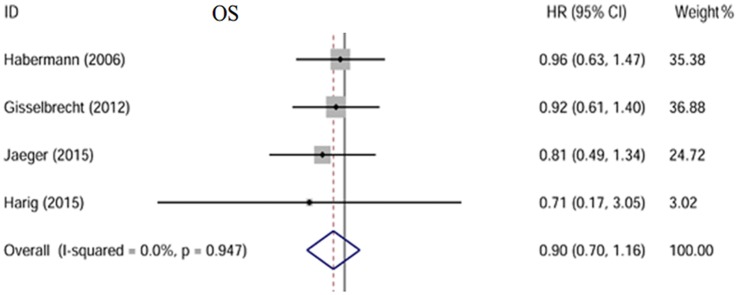
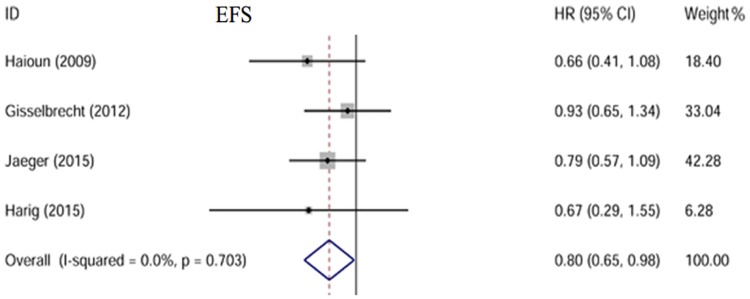
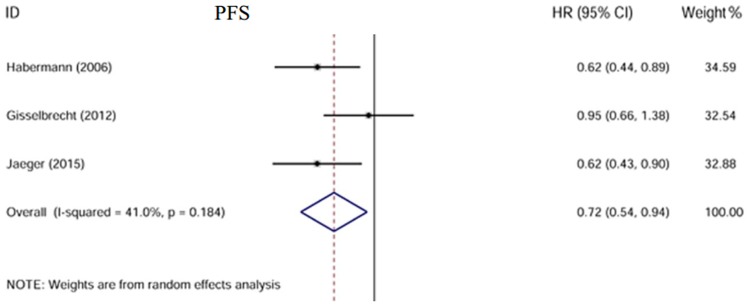
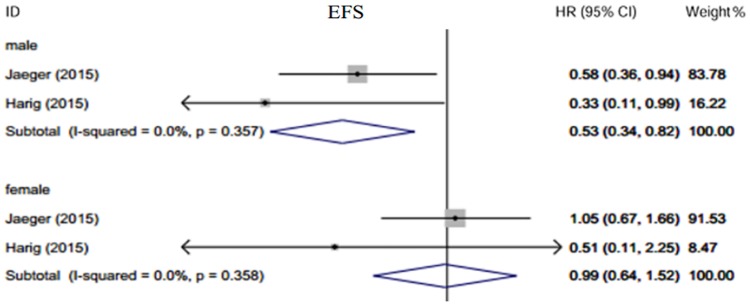
Totally 5 studies including 1740 patients were eligible for the meta-analysis. Compared to the observation group, patients who received rituximab maintenance therapy had significantly improved event-free survival (EFS) (HR = 0.80, 95% CI: 0.65-0.98) and progression-free survival (PFS) (HR = 0.72, 95% CI: 0.54-0.94). However, there was no statistically significant difference in overall survival (OS) (HR = 0.66, 95% CI: 0.27-1.29). A subgroup analysis suggested that male patients may benefit from rituximab maintenance therapy with a better EFS (HR = 0.53, 95% CI: 0.34-0.82-), while this advantage was not observed in female patients (HR = 0.99, 95% CI: 0.64-1.52).
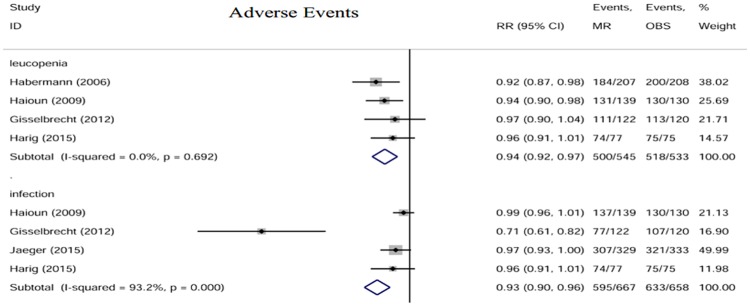
Rituximab maintenance may provide survival benefits beyond that afforded by first- and second-line chemotherapy alone, especially in male patients. However, maintenance rituximab treatment may cause more adverse events. It is recommended that both survival benefits and adverse events should be taken into consideration when making treatment decisions.
在标准化疗基础上加用利妥昔单抗已显著提高淋巴瘤患者的生存率。最近,利妥昔单抗维持治疗已被证明可预防滤泡性或套细胞淋巴瘤患者复发并带来生存获益。然而,利妥昔单抗对弥漫性大B细胞淋巴瘤(DLBCL)患者的疗效仍不明确。过去一年进行了两项涉及利妥昔单抗治疗DLBCL的新研究。我们进行了一项荟萃分析以评估利妥昔单抗维持治疗DLBCL患者的疗效。
检索了几个数据库(PubMed、MEDLINE、EMBASE和Cochrane对照试验中心注册库),以查找2016年5月之前发表的相关随机对照试验。两名评审员独立评估纳入研究的质量并提取数据。汇总并估计了事件发生时间数据的风险比(HRs)和其他数据的相对风险(RRs)。
共有5项研究(包括1740例患者)符合荟萃分析的条件。与观察组相比,接受利妥昔单抗维持治疗的患者无事件生存期(EFS)(HR = 0.80,95%CI:0.65 - 0.98)和无进展生存期(PFS)(HR = 0.72,95%CI:0.54 - 0.94)显著改善。然而,总生存期(OS)无统计学显著差异(HR = 0.66,95%CI:0.27 - 1.29)。亚组分析表明,男性患者可能从利妥昔单抗维持治疗中获益,EFS更好(HR = 0.53,95%CI:0.34 - 0.82),而女性患者未观察到这一优势(HR = 0.99,95%CI:0.64 - 1.52)。
利妥昔单抗维持治疗可能带来超出一线和二线单纯化疗的生存获益,尤其是在男性患者中。然而,利妥昔单抗维持治疗可能会导致更多不良事件。建议在做出治疗决策时同时考虑生存获益和不良事件。