Pierpont Timothy M, Limper Candice B, Richards Kristy L
Richards Laboratory, Department of Biomedical Sciences, Cornell University, Ithaca, NY, United States.
Department of Medicine, Sandra and Edward Meyer Cancer Center, Weill Cornell Medicine, New York, NY, United States.
Front Oncol. 2018 Jun 4;8:163. doi: 10.3389/fonc.2018.00163. eCollection 2018.
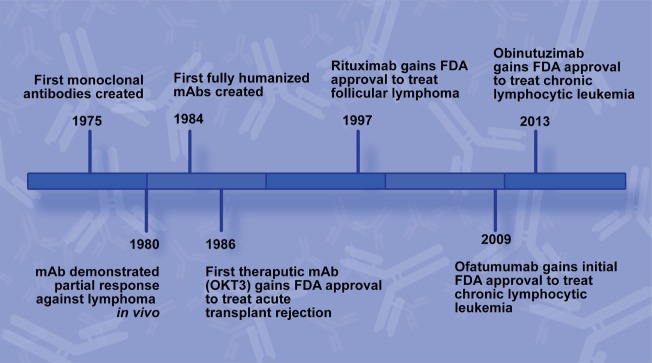
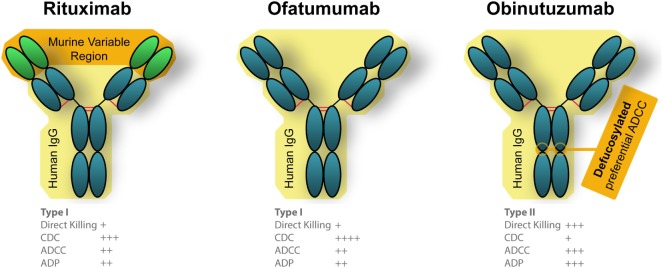
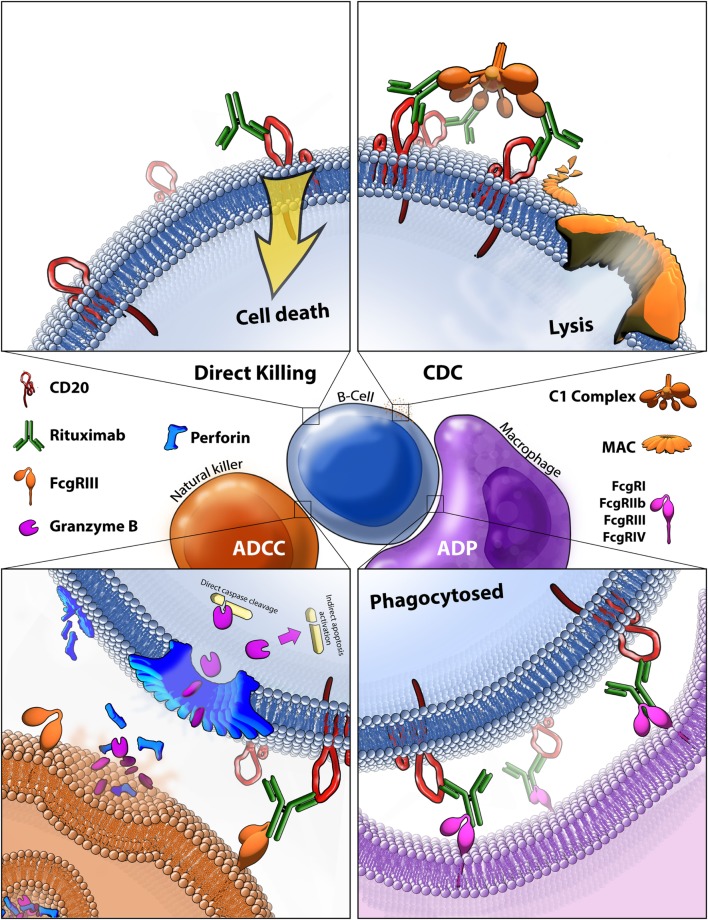
Rituximab is a chimeric mouse/human monoclonal antibody (mAb) therapy with binding specificity to CD20. It was the first therapeutic antibody approved for oncology patients and was the top-selling oncology drug for nearly a decade with sales reaching $8.58 billion in 2016. Since its initial approval in 1997, it has improved outcomes in all B-cell malignancies, including diffuse large B-cell lymphoma, follicular lymphoma, and chronic lymphocytic leukemia. Despite widespread use, most mechanistic data have been gathered from studies while the roles of the various response mechanisms in humans are still largely undetermined. Polymorphisms in Fc gamma receptor and complement protein genes have been implicated as potential predictors of differential response to rituximab, but have not yet shown sufficient influence to impact clinical decisions. Unlike most targeted therapies developed today, no known biomarkers to indicate target engagement/tumor response have been identified, aside from reduced tumor burden. The lack of companion biomarkers beyond CD20 itself has made it difficult to predict which patients will respond to any given anti-CD20 antibody. In the past decade, two new anti-CD20 antibodies have been approved: ofatumumab, which binds a distinct epitope of CD20, and obinutuzumab, a mAb derived from rituximab with modifications to the Fc portion and to its glycosylation. Both are fully humanized and have biological activity that is distinct from that of rituximab. In addition to these new anti-CD20 antibodies, another imminent change in targeted lymphoma treatment is the multitude of biosimilars that are becoming available as rituximab's patent expires. While the widespread use of rituximab itself will likely continue, its biosimilars will increase global access to the therapy. This review discusses current research into mechanisms and potential biomarkers of rituximab response, as well as its biosimilars and the newer CD20 binding mAb therapies. Increased ability to assess the effectiveness of rituximab in an individual patient, along with the availability of alternative anti-CD20 antibodies will likely lead to dramatic changes in how we use CD20 antibodies going forward.
利妥昔单抗是一种嵌合型鼠/人单克隆抗体(mAb)疗法,对CD20具有结合特异性。它是首个被批准用于肿瘤患者的治疗性抗体,近十年来一直是最畅销的肿瘤药物,2016年销售额达85.8亿美元。自1997年首次获批以来,它改善了所有B细胞恶性肿瘤的治疗效果,包括弥漫性大B细胞淋巴瘤、滤泡性淋巴瘤和慢性淋巴细胞白血病。尽管已广泛使用,但大多数机制数据是从研究中收集的,而各种反应机制在人类中的作用仍很大程度上未确定。Fcγ受体和补体蛋白基因的多态性被认为是对利妥昔单抗反应差异的潜在预测指标,但尚未显示出足以影响临床决策的影响。与当今开发的大多数靶向疗法不同,除了肿瘤负担减轻外,尚未发现已知的生物标志物来指示靶点结合/肿瘤反应。除了CD20本身之外,缺乏伴随生物标志物使得难以预测哪些患者会对任何给定的抗CD20抗体产生反应。在过去十年中,两种新的抗CD20抗体已被批准:奥法木单抗,它结合CD20的一个独特表位;奥妥珠单抗,一种源自利妥昔单抗的单克隆抗体,对Fc部分及其糖基化进行了修饰。两者都是完全人源化的,并且具有与利妥昔单抗不同的生物学活性。除了这些新的抗CD20抗体外,靶向淋巴瘤治疗的另一个即将到来的变化是随着利妥昔单抗专利到期,众多生物类似药即将上市。虽然利妥昔单抗本身可能会继续广泛使用,但其生物类似药将增加全球对该疗法的可及性。本综述讨论了利妥昔单抗反应机制和潜在生物标志物的当前研究,以及其生物类似药和更新的CD20结合单克隆抗体疗法。评估利妥昔单抗在个体患者中有效性的能力增强,以及替代抗CD20抗体的可用性,可能会导致我们未来使用CD20抗体的方式发生巨大变化。