He Chao-Bin, Lin Xiao-Jun
Department of Hepatobiliary Oncology, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, Guangdong, P.R. China.
PLoS One. 2017 Mar 29;12(3):e0174769. doi: 10.1371/journal.pone.0174769. eCollection 2017.
The systemic inflammatory response plays an important role in cancer development and progression. An original inflammation-based staging system for predicting survival in patients undergoing transarterial chemoembolization (TACE) combined with recombinant human type-5 adenovirus H101 is not available. This study aimed to validate the prognostic value of inflammation scores for patients with hepatocellular carcinoma (HCC) who were treated with TACE combined with H101.
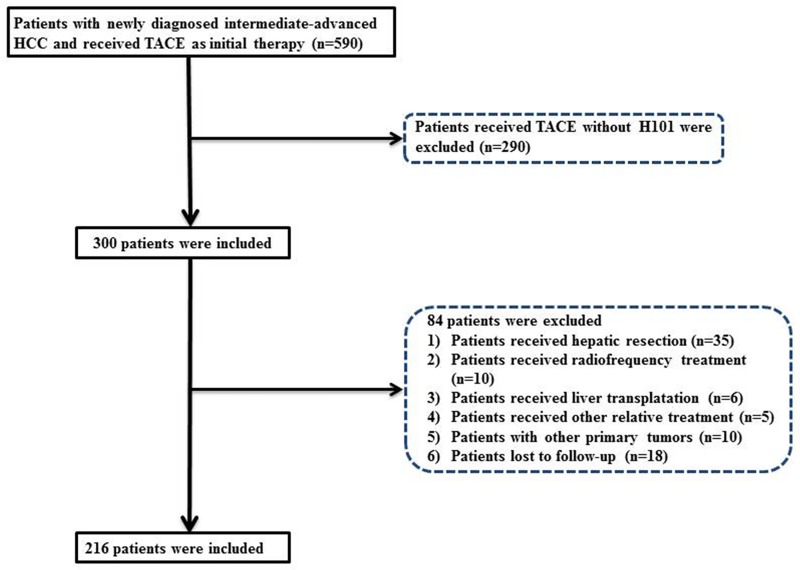
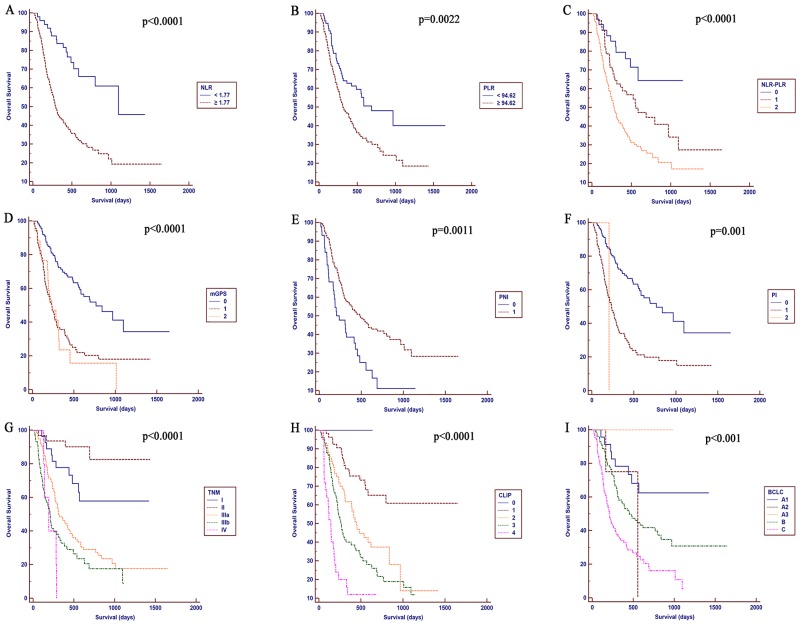
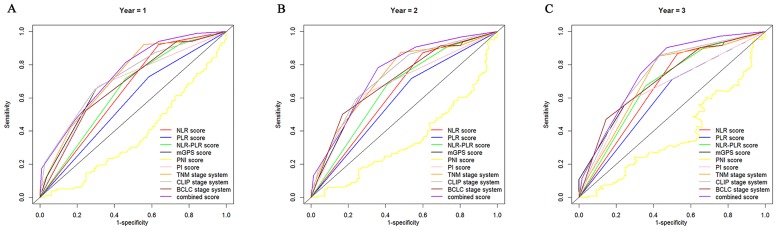
The data from 216 patients with HCC who underwent TACE combined with H101 from January 2007 to July 2015 were retrospectively collected, and the association of the inflammation scores with overall survival (OS) was analyzed. Univariate and multivariate analyses were performed to identify variables associated with OS. The prognostic value of the inflammation scores, including the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), neutrophil/ platelet-to-lymphocyte ratio (NLR-PLR), modified Glasgow Prognostic Score (mGPS), prognostic nutritional index (PNI), prognostic index (PI), tumor-node-metastasis (TNM), Barcelona Clinic Liver Cancer (BCLC) and Cancer of the Liver Italian Program (CLIP) staging systems were analyzed and compared using the areas under the receiver operating characteristic curves (AUROCs).
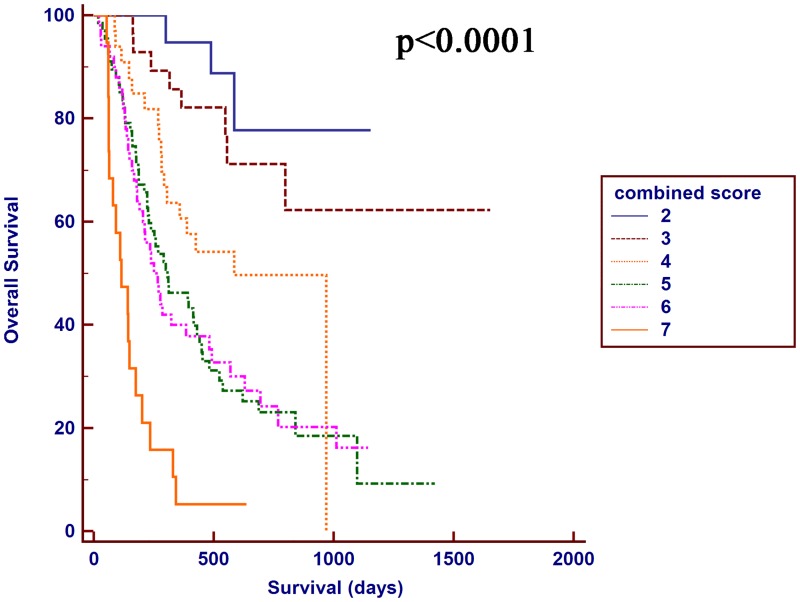
The estimated 1-, 2-, and 3-year OS rates were 61.3%, 44.2%, and 40.5% for the entire study cohort, respectively; the median OS was 17 months. According to the multivariate Cox proportional hazards model, the pretreatment NLR, tumor diameter and pretreatment alpha-fetoprotein (AFP) levels were independent predictors of OS. The CLIP score had superior discriminative abilities compared with other staging systems, and the NLR-PLR score consistently displayed a higher AUROC value than the other inflammation-based prognostic scores. The combination of the NLR-PLR and CLIP scores exhibited a superior prognostic ability for OS compared to the NLR-PLR or CLIP scores alone.
The NLR-PLR score is a more powerful predictive system than the other inflammation-based scores for patients with HCC who were treated with TACE and H101. The predictive ability may be improved by utilizing a combination of the NLR-PLR and CLIP scores.
全身炎症反应在癌症的发生和发展中起着重要作用。目前尚无基于炎症的原创分期系统来预测接受经动脉化疗栓塞术(TACE)联合重组人5型腺病毒H101治疗患者的生存率。本研究旨在验证炎症评分对接受TACE联合H101治疗的肝细胞癌(HCC)患者的预后价值。
回顾性收集2007年1月至2015年7月期间216例接受TACE联合H101治疗的HCC患者的数据,并分析炎症评分与总生存期(OS)的相关性。进行单因素和多因素分析以确定与OS相关的变量。使用受试者工作特征曲线下面积(AUROC)分析并比较炎症评分的预后价值,包括中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)、中性粒细胞/血小板与淋巴细胞比值(NLR-PLR)、改良格拉斯哥预后评分(mGPS)、预后营养指数(PNI)、预后指数(PI)、肿瘤-淋巴结-转移(TNM)、巴塞罗那临床肝癌(BCLC)和意大利肝癌项目(CLIP)分期系统。
整个研究队列的1年、2年和3年OS率估计分别为61.3%、44.2%和40.5%;中位OS为17个月。根据多因素Cox比例风险模型,治疗前NLR、肿瘤直径和治疗前甲胎蛋白(AFP)水平是OS的独立预测因素。与其他分期系统相比,CLIP评分具有更好的判别能力,并且NLR-PLR评分始终显示出比其他基于炎症的预后评分更高的AUROC值。与单独的NLR-PLR或CLIP评分相比,NLR-PLR和CLIP评分的组合对OS表现出更好的预后能力。
对于接受TACE和H101治疗的HCC患者,NLR-PLR评分是比其他基于炎症的评分更强大的预测系统。通过联合使用NLR-PLR和CLIP评分,预测能力可能会得到提高。