Huang Shao-Hong, Kong Qing-Lei, Chen Xue-Xia, He Jin-Yuan, Qin Jie, Chen Zhuang-Gui
Department of Cardiothoracic Surgery, The Third Affiliated Hospital, Sun Yat-sen University, Guangzhou, China.
Department of Emergency, the Third Affiliated Hospital, Sun Yat-sen University, Guangzhou, China.
Ther Clin Risk Manag. 2017 Mar 23;13:355-360. doi: 10.2147/TCRM.S130264. eCollection 2017.
Several case reports and studies have suggested that there is an increased survival rate for patients who undergo resection of solitary adrenal metastasis from non-small cell lung cancer (NSCLC). This study aimed to investigate whether NSCLC patients with solitary adrenal metastasis could gain a higher survival rate after adrenalectomy (ADX) when compared with those patients undergoing nonsurgical treatment, and to investigate the potential prognostic factors.
A total of 1,302 NSCLC inpatients' data from 2001 to 2015 were retrospectively reviewed to identify those with solitary adrenal metastasis. Overall survival for those who underwent both primary resection and ADX was compared to those patients with conservative treatment using the log-rank test. Potential prognostic variables were evaluated with univariate and multivariate analyses including clinical, therapeutic, pathologic, primary and metastatic data.
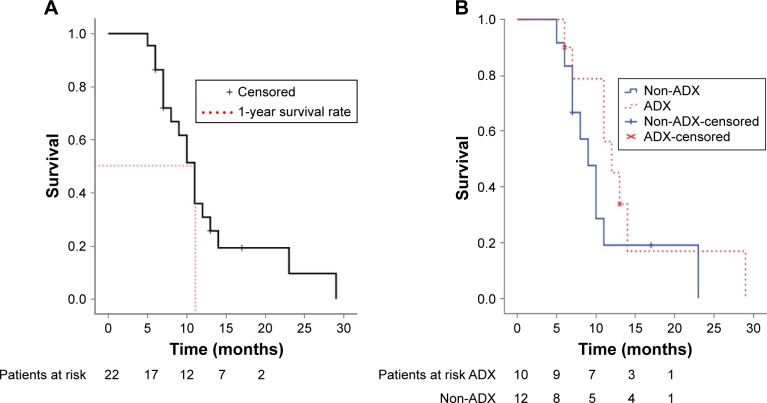
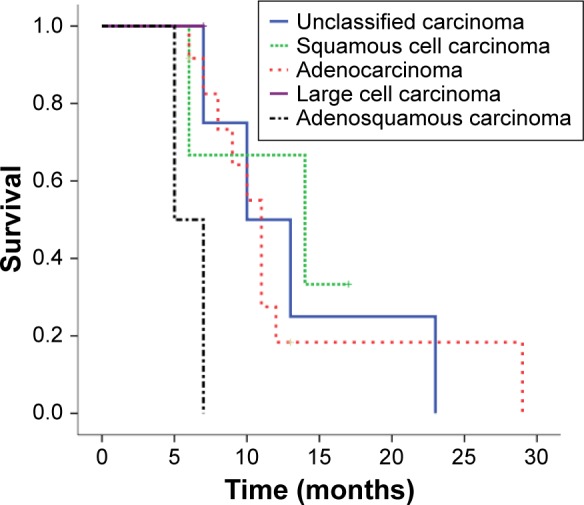
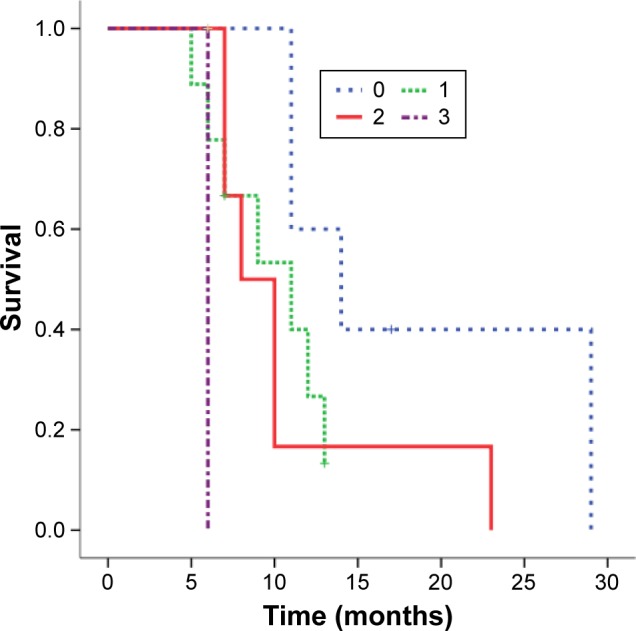
A total of 22 NSCLC patients with solitary adrenal metastasis were identified, with an overall median survival of 11 months (95% confidence interval: 9.4-12.6 months) and a 1-year survival rate of 51.4% (95% confidence interval: 29.6%-73.2%). All of the patients had died by 30 months. There was no significant survival difference between patients who underwent primary and metastasis resection (n=10) and those treated conservatively (n=12), (=0.209). Univariate analysis identified Eastern Cooperative Oncology Group performance status (ECOG PS) as the significant predictor of survival (=0.024). Age (<65 vs ≥65 years), sex, pathologic type, mediastinal lymph node stage (N2 vs N0/N1), primary tumor size (<5 vs ≥5 cm), primary location (central vs peripheral), metastatic tumor size (<5 vs ≥5 cm), metastasis laterality, synchronous metastasis, and metastatic field radiotherapy were not identified as potential prognostic factors in relation to survival rate. In multivariate analysis, a stepwise selection procedure allowed both ECOG PS (=0.007, relative risk =3.57) and pathologic type (=0.069) to enter the Cox's hazard function.
Primary and metastatic radical resection may not prolong the survival of NSCLC patients with solitary adrenal metastasis. ECOG PS and pathologic type might be the prognostic factors for these patients.
多项病例报告和研究表明,接受非小细胞肺癌(NSCLC)孤立性肾上腺转移灶切除术的患者生存率有所提高。本研究旨在探讨与接受非手术治疗的患者相比,NSCLC孤立性肾上腺转移患者肾上腺切除术(ADX)后是否能获得更高的生存率,并探讨潜在的预后因素。
回顾性分析2001年至2015年共1302例NSCLC住院患者的数据,以确定那些有孤立性肾上腺转移的患者。使用对数秩检验比较接受原发灶切除和ADX的患者与保守治疗患者的总生存期。通过单因素和多因素分析评估潜在的预后变量,包括临床、治疗、病理、原发和转移数据。
共确定22例NSCLC孤立性肾上腺转移患者,总中位生存期为11个月(95%置信区间:9.4 - 12.6个月),1年生存率为51.4%(95%置信区间:29.6% - 73.2%)。所有患者均在30个月内死亡。接受原发灶和转移灶切除的患者(n = 10)与保守治疗的患者(n = 12)之间的生存率无显著差异(P = 0.209)。单因素分析确定东部肿瘤协作组体能状态(ECOG PS)是生存的显著预测因素(P = 0.024)。年龄(<65岁与≥岁)、性别、病理类型、纵隔淋巴结分期(N2与N0/N1)、原发肿瘤大小(<5 cm与≥5 cm)、原发部位(中央与周围)、转移肿瘤大小(<5 cm与≥5 cm)、转移侧别、同步转移和转移野放疗未被确定为与生存率相关的潜在预后因素。在多因素分析中,逐步选择程序允许ECOG PS(P = 0.007,相对风险 = 3.57)和病理类型(P = 0.069)进入Cox风险函数。
原发灶和转移灶根治性切除可能不会延长NSCLC孤立性肾上腺转移患者的生存期。ECOG PS和病理类型可能是这些患者的预后因素。