van Geel Robin M J M, Tabernero Josep, Elez Elena, Bendell Johanna C, Spreafico Anna, Schuler Martin, Yoshino Takayuki, Delord Jean-Pierre, Yamada Yasuhide, Lolkema Martijn P, Faris Jason E, Eskens Ferry A L M, Sharma Sunil, Yaeger Rona, Lenz Heinz-Josef, Wainberg Zev A, Avsar Emin, Chatterjee Arkendu, Jaeger Savina, Tan Eugene, Maharry Kati, Demuth Tim, Schellens Jan H M
The Netherlands Cancer Institute, Amsterdam, the Netherlands.
Vall d'Hebron University Hospital and Institute of Oncology (VHIO), Universitat Autònoma de Barcelona, Barcelona, Spain.
Cancer Discov. 2017 Jun;7(6):610-619. doi: 10.1158/2159-8290.CD-16-0795. Epub 2017 Mar 31.
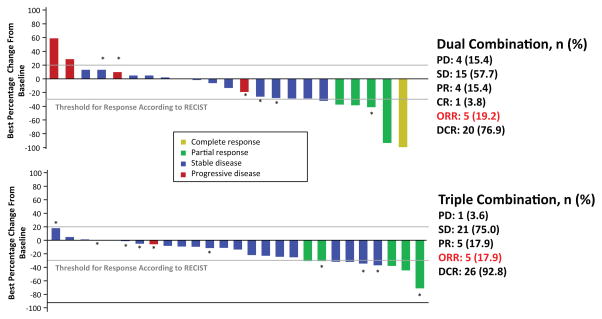
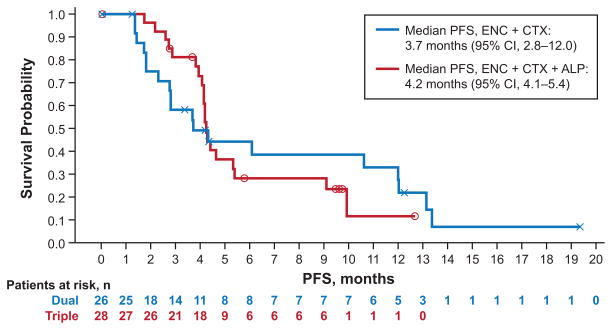
Preclinical evidence suggests that concomitant BRAF and EGFR inhibition leads to sustained suppression of MAPK signaling and suppressed tumor growth in colorectal cancer models. Patients with refractory -mutant metastatic CRC (mCRC) were treated with a selective RAF kinase inhibitor (encorafenib) plus a monoclonal antibody targeting EGFR (cetuximab), with ( = 28) or without ( = 26) a PI3Kα inhibitor (alpelisib). The primary objective was to determine the maximum tolerated dose (MTD) or a recommended phase II dose. Dose-limiting toxicities were reported in 3 patients receiving dual treatment and 2 patients receiving triple treatment. The MTD was not reached for either group and the phase II doses were selected as 200 mg encorafenib (both groups) and 300 mg alpelisib. Combinations of cetuximab and encorafenib showed promising clinical activity and tolerability in patients with -mutant mCRC; confirmed overall response rates of 19% and 18% were observed and median progression-free survival was 3.7 and 4.2 months for the dual- and triple-therapy groups, respectively. Herein, we demonstrate that dual- (encorafenib plus cetuximab) and triple- (encorafenib plus cetuximab and alpelisib) combination treatments are tolerable and provide promising clinical activity in the difficult-to-treat patient population with -mutant mCRC. .
临床前证据表明,在结直肠癌模型中,同时抑制BRAF和EGFR可导致MAPK信号通路的持续抑制和肿瘤生长的抑制。难治性BRAF突变转移性结直肠癌(mCRC)患者接受了选择性RAF激酶抑制剂(恩考芬尼)加靶向EGFR的单克隆抗体(西妥昔单抗)治疗,其中28例联合PI3Kα抑制剂(阿培利司),26例未联合。主要目的是确定最大耐受剂量(MTD)或推荐的II期剂量。接受双联治疗的3例患者和接受三联治疗的2例患者报告了剂量限制性毒性。两组均未达到MTD,II期剂量选定为恩考芬尼200mg(两组)和阿培利司300mg。西妥昔单抗和恩考芬尼联合用药在BRAF突变mCRC患者中显示出有前景的临床活性和耐受性;双联和三联治疗组的确认总缓解率分别为19%和18%,中位无进展生存期分别为3.7个月和4.2个月。在此,我们证明双联(恩考芬尼加西妥昔单抗)和三联(恩考芬尼加西妥昔单抗和阿培利司)联合治疗在BRAF突变mCRC这一难治性患者群体中耐受性良好,并具有有前景的临床活性。