Lopez Régis, Barateau Lucie, Evangelista Elisa, Chenini Sofiene, Robert Philippe, Jaussent Isabelle, Dauvilliers Yves
Unité des Troubles du Sommeil Service de Neurologie, Centre National de Référence Narcolepsie Hypersomnies, Hôpital Gui-de-Chauliac, Montpellier F-34000, France.
Inserm U1061, Montpellier F-34000, France.
Sleep. 2017 Jan 1;40(1). doi: 10.1093/sleep/zsw010.
To follow the temporal changes of cerebrospinal fluid (CSF) biomarker levels in narcoleptic patients with unexpected hypocretin level at referral.
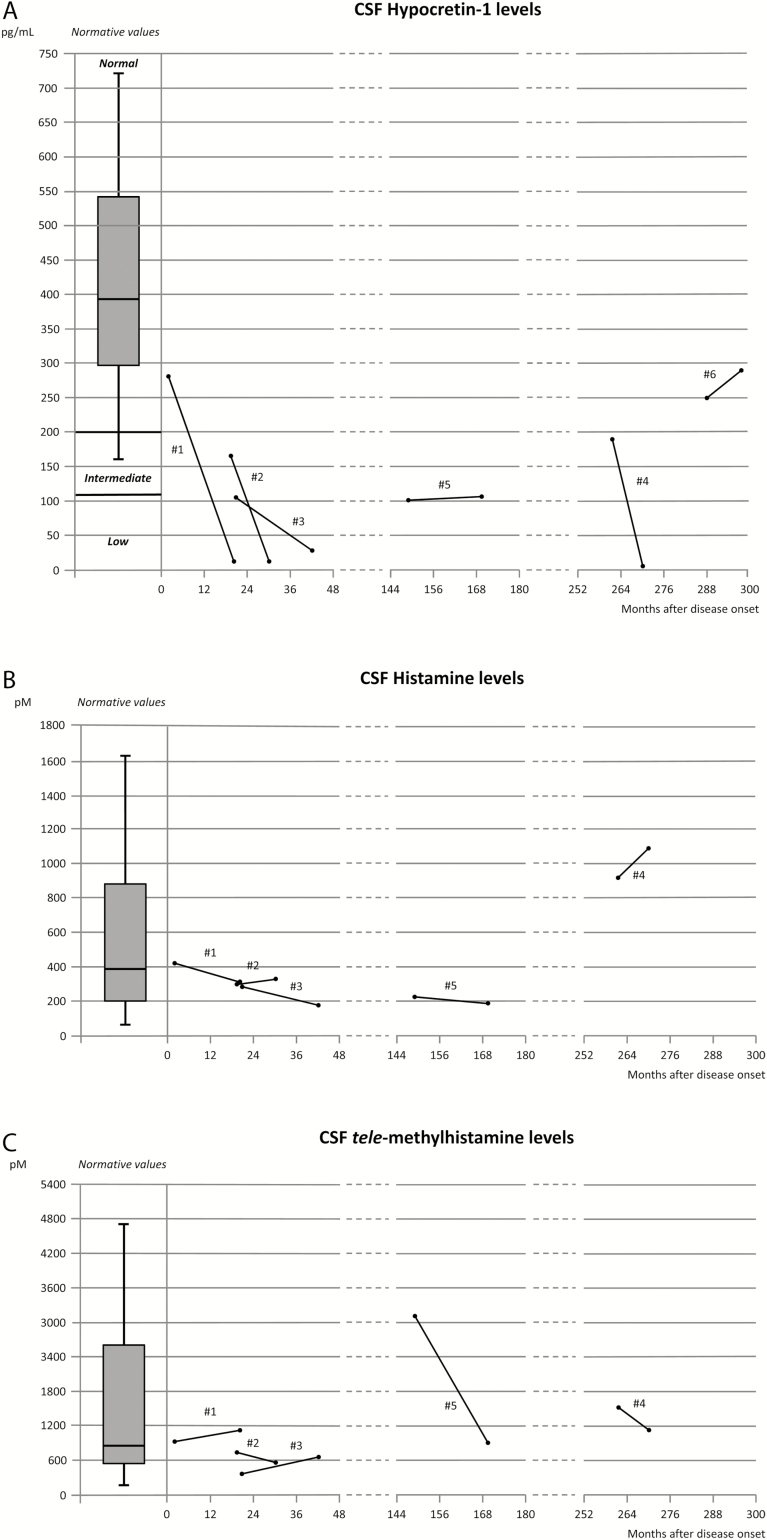
From 2007 to 2015, 170 human leukocyte antigen (HLA) DQB1*06:02-positive patients with primary narcolepsy and definite (n = 155, 95 males, 60 females, 36 children) or atypical cataplexy (n = 15, 4 males, 3 children) were referred to our center. Cerebrospinal hypocretin deficiency was found in 95.5% and 20% of patients with definitive and atypical cataplexy, respectively. CSF hypocretin-1 (n = 6) and histamine/tele-methylhistamine (n = 5) levels were assessed twice (median interval: 14.4 months) in four patients with definite and in two with atypical cataplexy and hypocretin level greater than 100 pg/mL at baseline.
CSF hypocretin levels decreased from normal/intermediate to undetectable levels in three of the four patients with definite cataplexy and remained stable in the other (>250 pg/mL). Hypocretin level decreased from 106 to 27 pg/mL in one patient with atypical cataplexy, and remained stable in the other (101 and 106 pg/mL). CSF histamine and tele-methylhistamine levels remained stable, but for one patient showing increased frequency of cataplexy and a strong decrease (-72.5%) of tele-methylhistamine levels several years after disease onset. No significant association was found between relative or absolute change in hypocretin level and demographic/clinical features.
These findings show that in few patients with narcolepsy with cataplexy, symptoms and CSF marker levels can change over time. In these rare patients with cataplexy without baseline hypocretin deficiency, CSF markers should be monitored over time with potential for immune therapies in early stages to try limiting hypocretin neuron loss.
追踪转诊时脑脊液中下丘脑分泌素水平异常的发作性睡病患者脑脊液生物标志物水平随时间的变化。
2007年至2015年,170例人类白细胞抗原(HLA)DQB1*06:02阳性的原发性发作性睡病患者被转诊至本中心,其中明确猝倒发作的患者155例(男性95例,女性60例,儿童36例),非典型猝倒发作的患者15例(男性4例,儿童3例)。明确猝倒发作和非典型猝倒发作的患者中,脑脊液下丘脑分泌素缺乏分别占95.5%和20%。对4例明确猝倒发作且基线下丘脑分泌素水平大于100 pg/mL的患者以及2例非典型猝倒发作且下丘脑分泌素水平大于100 pg/mL的患者,评估了两次脑脊液下丘脑分泌素-1水平(n = 6)和组胺/3-甲基组胺水平(n = 5)(中位间隔时间:14.4个月)。
4例明确猝倒发作的患者中,有3例脑脊液下丘脑分泌素水平从正常/中等水平降至无法检测到的水平,另一例保持稳定(>250 pg/mL)。1例非典型猝倒发作的患者下丘脑分泌素水平从106 pg/mL降至27 pg/mL,另一例保持稳定(101和106 pg/mL)。脑脊液组胺和3-甲基组胺水平保持稳定,但有1例患者在疾病发作数年之后猝倒发作频率增加,3-甲基组胺水平大幅下降(-72.5%)。下丘脑分泌素水平的相对或绝对变化与人口统计学/临床特征之间未发现显著关联。
这些研究结果表明,在少数伴有猝倒发作的发作性睡病患者中,症状和脑脊液标志物水平会随时间变化。在这些罕见的无基线下丘脑分泌素缺乏的猝倒发作患者中,应随时间监测脑脊液标志物,以便在早期阶段进行免疫治疗,尝试限制下丘脑分泌素神经元的损失。