Sáez-Llorens Xavier, Rowley Stella, Wong Digna, Rodríguez Mirna, Calvo Arlene, Troitiño Marisol, Salas Albino, Vega Vielka, Castrejón Maria Mercedes, Lommel Patricia, Pascal Thierry G, Hausdorff William P, Borys Dorota, Ruiz-Guiñazú Javier, Ortega-Barría Eduardo, Yarzabal Juan Pablo, Schuerman Lode
a Department of Infectious Diseases , Hospital del Niño, Panama City, Panama; Distinguished Member of the SNI , Senacyt , Panama.
b Department of Otorhinolaryngology Hospital del Niño , Panama City , Panama.
Hum Vaccin Immunother. 2017 Jun 3;13(6):1-16. doi: 10.1080/21645515.2017.1287640. Epub 2017 Feb 25.
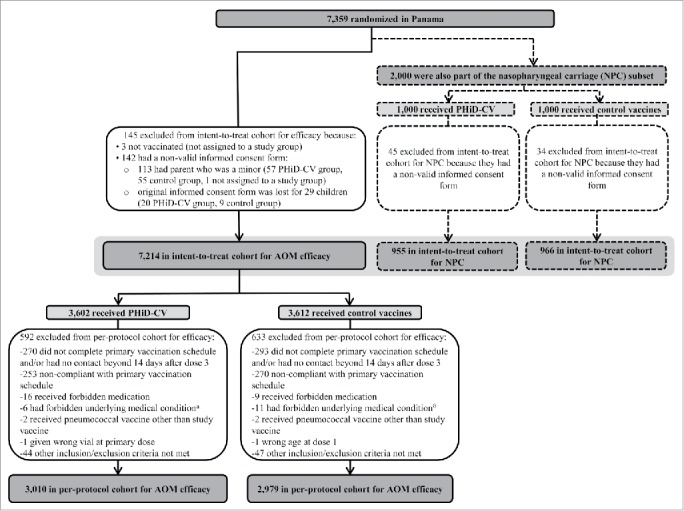
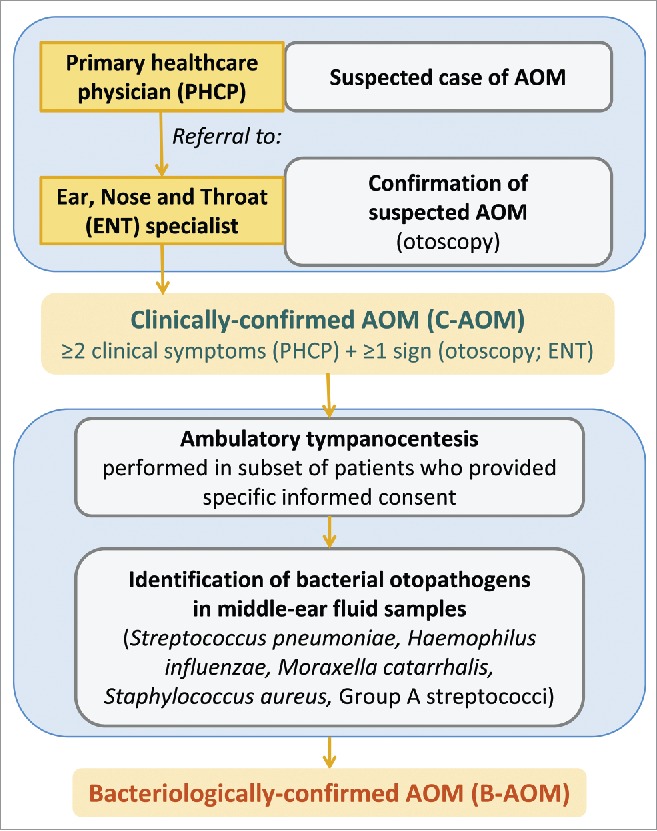
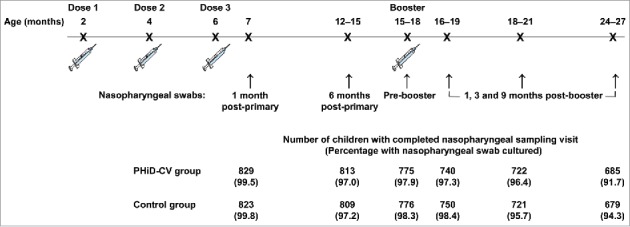
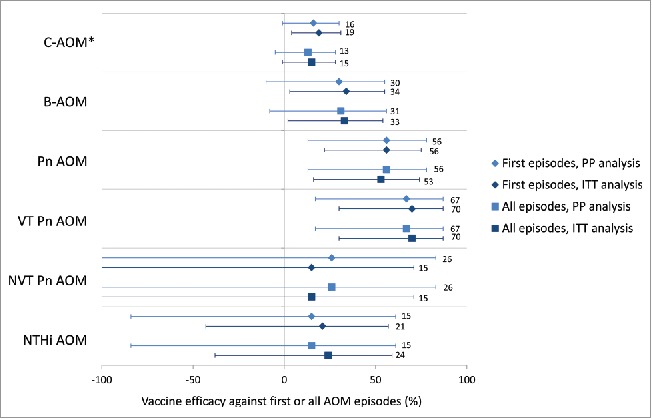
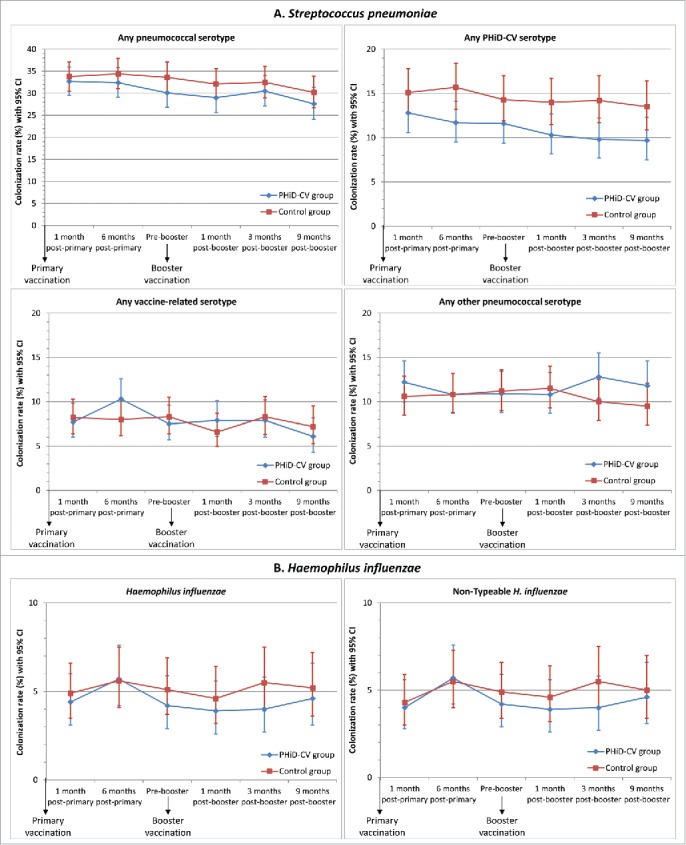
We previously reported 10-valent pneumococcal non-typeable Haemophilus influenzae (NTHi) protein D conjugate vaccine (PHiD-CV) efficacy in a double-blind randomized trial (ClinicalTrials.gov: NCT00466947) against various diseases, including acute otitis media (AOM). Here, we provide further analyses. In the Panamanian subset, 7,359 children were randomized (1:1) to receive PHiD-CV or control vaccine at age 2/4/6 and 15-18 months. Of these, 2,000 had nasopharyngeal swabs collected. AOM cases were captured when parents sought medical attention for children with AOM symptoms; surveillance was enhanced approximately 2 y into the study through regular telephone calls or home visits by study personnel, who advised parents to visit the clinic if their child had AOM symptoms. Mean follow-up was 31.4 months. Clinical AOM (C-AOM) cases were assessed by physicians and confirmed by otorhinolaryngologists. Middle ear fluid samples, taken from children with C-AOM after specific informed consent, and nasopharyngeal samples were cultured for pathogen identification. For 7,359 children, 2,574 suspected AOM cases were assessed by a primary healthcare physician; 649 cases were C-AOM cases as per protocol definition. From the 503 MEF samples collected, 158 resulted in a positive culture. In the intent-to-treat cohort (7,214 children), PHiD-CV showed VE against first C-AOM (24.0% [95% CI: 8.7, 36.7]) and bacterial (B-AOM) episodes (48.0% [20.3, 66.1]) in children <24 months, which declined thereafter with age. Pre-booster VE against C-AOM was 30.7% [12.9, 44.9]; post-booster, -6.7% [-36.4, 16.6]. PHiD-CV VE was 17.7% [-6.1, 36.2] against moderate and 32.7% [-20.5, 62.4] against severe C-AOM. VE against vaccine-serotype pneumococcal NPC was 31.2% [5.3, 50.3] 3 months post-booster, and 25.6% [12.7, 36.7] across all visits. NTHi colonization rates were low and no significant reduction was observed. PHiD-CV showed efficacy against C-AOM and B-AOM in children younger than 24 months, and reduced vaccine-serotype NPC.
我们之前在一项双盲随机试验(ClinicalTrials.gov:NCT00466947)中报告了10价肺炎球菌非分型流感嗜血杆菌(NTHi)蛋白D结合疫苗(PHiD-CV)针对包括急性中耳炎(AOM)在内的多种疾病的疗效。在此,我们提供进一步分析。在巴拿马亚组中,7359名儿童被随机分组(1:1),在2/4/6月龄和15 - 18月龄时接受PHiD-CV或对照疫苗。其中,2000名儿童采集了鼻咽拭子。当家长因孩子出现AOM症状寻求医疗帮助时捕获AOM病例;在研究进行约2年时,通过研究人员定期电话随访或家访加强监测,研究人员建议家长如果孩子有AOM症状就带其去诊所就诊。平均随访时间为31.4个月。临床AOM(C-AOM)病例由医生评估,并经耳鼻喉科医生确诊。在获得特定知情同意后,从患有C-AOM的儿童中采集中耳积液样本,并对鼻咽样本进行病原体培养鉴定。对于7359名儿童,初级保健医生评估了2574例疑似AOM病例;根据方案定义,649例为C-AOM病例。从采集的503份中耳积液样本中,158份培养结果为阳性。在意向性治疗队列(7214名儿童)中,PHiD-CV在24个月以下儿童中针对首次C-AOM显示出疫苗效力(VE)为24.0%[95%CI:8.7,36.7]),针对细菌性(B-AOM)发作的VE为48.0%[20.3,66.1]),此后随年龄下降。加强免疫前针对C-AOM的VE为30.7%[12.9,44.9];加强免疫后为 - 6.7%[-36.4,16.6]。PHiD-CV针对中度C-AOM的VE为17.7%[-6.1,36.2],针对重度C-AOM的VE为32.7%[-20.5,62.4]。加强免疫后3个月针对疫苗血清型肺炎球菌鼻咽携带(NPC)的VE为31.2%[5.3,50.3],在所有访视中为25.6%[12.7,36.7]。NTHi定植率较低,未观察到显著降低。PHiD-CV在24个月以下儿童中针对C-AOM和B-AOM显示出疗效,并降低了疫苗血清型NPC。