Steinbuch J, van Dijk A C, Schreuder Fhbm, Truijman Mtb, Hendrikse J, Nederkoorn P J, van der Lugt A, Hermeling E, Hoeks Apg, Mess W H
Biomedical Engineering, Cardiovascular Research Institute Maastricht, Maastricht University, Maastricht, The Netherlands.
Radiology, Erasmus Medical Center, Rotterdam, The Netherlands.
Cardiovasc Ultrasound. 2017 Apr 4;15(1):9. doi: 10.1186/s12947-017-0097-4.
Mean or maximal intima-media thickness (IMT) is commonly used as surrogate endpoint in intervention studies. However, the effect of normalization by surrounding or median IMT or by diameter is unknown. In addition, it is unclear whether IMT inhomogeneity is a useful predictor beyond common wall parameters like maximal wall thickness, either absolute or normalized to IMT or lumen size. We investigated the interrelationship of common carotid artery (CCA) thickness parameters and their association with the ipsilateral internal carotid artery (ICA) stenosis degree.
CCA thickness parameters were extracted by edge detection applied to ultrasound B-mode recordings of 240 patients. Degree of ICA stenosis was determined from CT angiography.
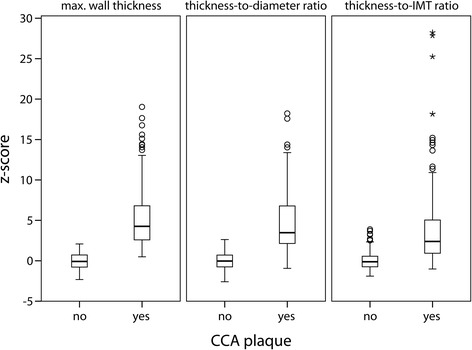
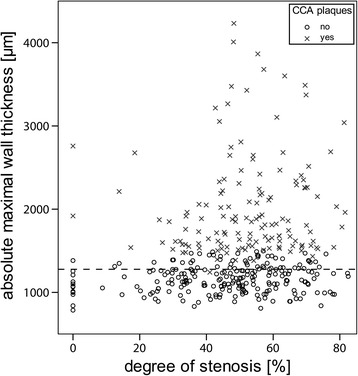
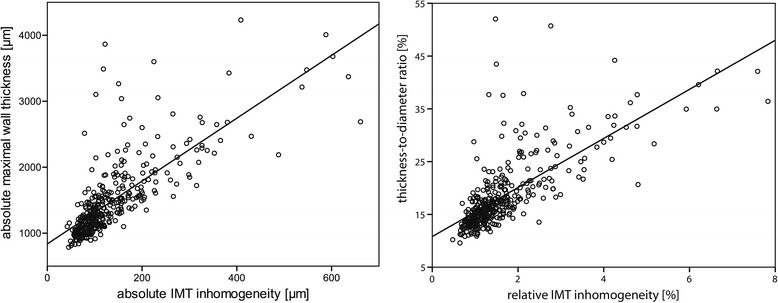
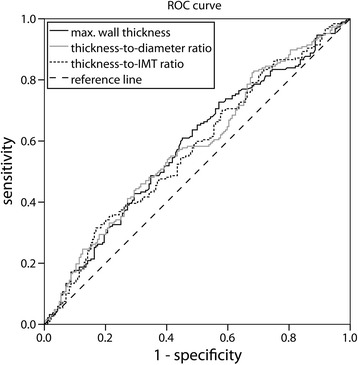
Normalization of maximal CCA wall thickness to median IMT leads to large variations. Higher CCA thickness parameter values are associated with a higher degree of ipsilateral ICA stenosis (p < 0.001), though IMT inhomogeneity does not provide extra information. When the ratio of wall thickness and diameter instead of absolute maximal wall thickness is used as risk marker for having moderate ipsilateral ICA stenosis (>50%), 55 arteries (15%) are reclassified to another risk category.
It is more reasonable to normalize maximal wall thickness to end-diastolic diameter rather than to IMT, affecting risk classification and suggesting modification of the Mannheim criteria.
Clinical trials.gov NCT01208025 .
平均或最大内膜中层厚度(IMT)通常在干预研究中用作替代终点。然而,通过周围或中位数IMT或直径进行标准化的效果尚不清楚。此外,IMT不均匀性是否是除最大壁厚等常见壁参数(无论是绝对的还是相对于IMT或管腔大小进行标准化)之外的有用预测指标尚不清楚。我们研究了颈总动脉(CCA)厚度参数之间的相互关系及其与同侧颈内动脉(ICA)狭窄程度的关联。
通过对240例患者的超声B模式记录应用边缘检测来提取CCA厚度参数。从CT血管造影确定ICA狭窄程度。
将最大CCA壁厚度标准化为中位数IMT会导致较大差异。较高的CCA厚度参数值与同侧ICA较高程度的狭窄相关(p < 0.001),尽管IMT不均匀性并未提供额外信息。当使用壁厚与直径的比值而非绝对最大壁厚作为同侧ICA中度狭窄(>50%)的风险标志物时,55条动脉(15%)被重新分类到另一个风险类别。
将最大壁厚度标准化为舒张末期直径而非IMT更为合理,这会影响风险分类并提示修改曼海姆标准。
ClinicalTrials.gov NCT01208025 。