Zhao Ya-Chao, Zhang Jia, Wang Fei, He Yi-Ming, Xu Ming-Jun, Wang Dong-Hai, Zhang Mei
National Key Laboratory for Innovation and Transformation of Luobing Theory, The Key Laboratory of Cardiovascular Remodeling and Function Research, Chinese Ministry of Education, Chinese National Health Commission and Chinese Academy of Medical Sciences, Department of Cardiology, Qilu Hospital of Shandong University, Jinan, China.
Neurosurgery Department, Qilu Hospital of Shandong University, Jinan, China.
Quant Imaging Med Surg. 2024 Feb 1;14(2):1994-2007. doi: 10.21037/qims-23-1193. Epub 2024 Jan 23.
Research has shown that carotid intima-media thickness (CIMT) could help to predict carotid plaque (CP) progression in patients with mild carotid stenosis. However, the debate continues as to the value of carotid intima thickness (CIT) in monitoring the development of CP in patients with severe carotid stenosis. This study sought to evaluate the relationships between CIT and the ultrasonic characteristics of CP and to analyze the value of CIT and the ultrasonic parameters of CP in assessing plaque vulnerability in advanced human carotid atherosclerosis.
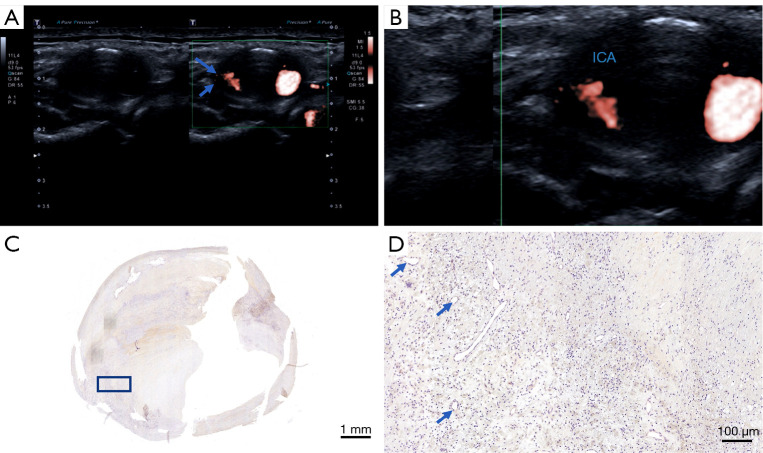
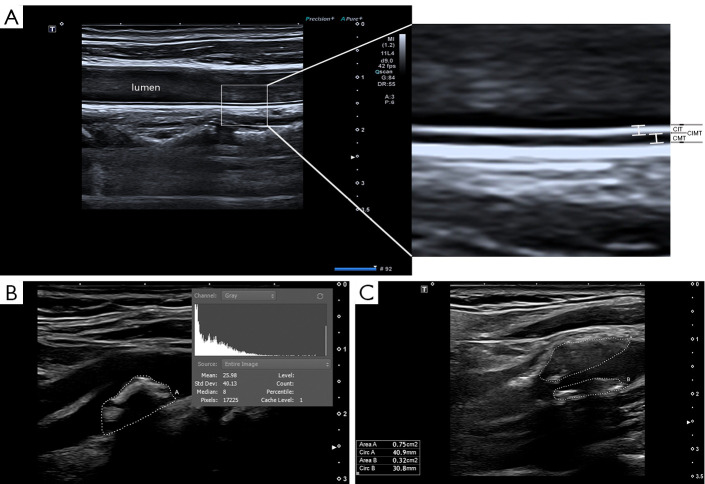
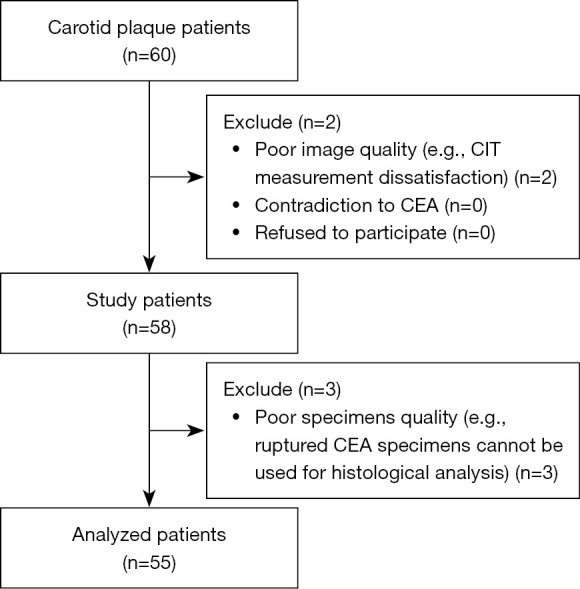
A total of 55 individuals who underwent carotid endarterectomy (CEA) were included in the study (mean age: 65±7 years; female: 9.1%). CIMT and CIT were examined at the common carotid artery (CCA). Plaque textural features, such as the gray-scale median (GSM), superb microvascular imaging (SMI) level, and total plaque area (TPA), were also identified. A Spearman correlation coefficient analysis was performed to examine the relationship between CIT and the ultrasonic parameters of CP. The CIT of various plaque types was compared. Receiver operating characteristic (ROC) curves were used to analyze the diagnostic values of the ultrasound characteristics to evaluate CP vulnerability.
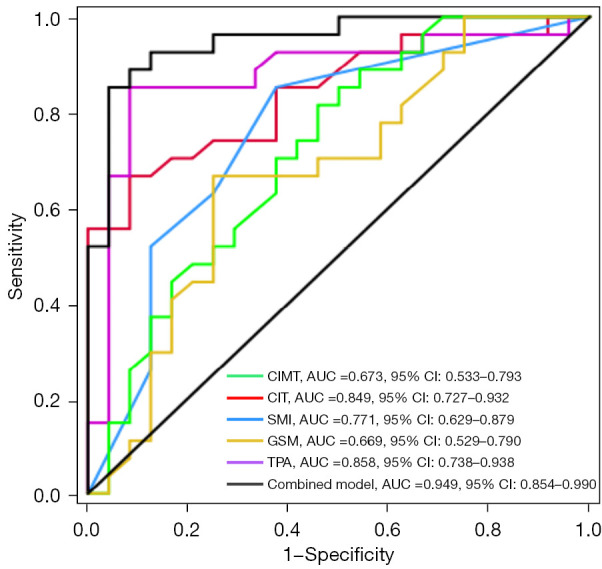
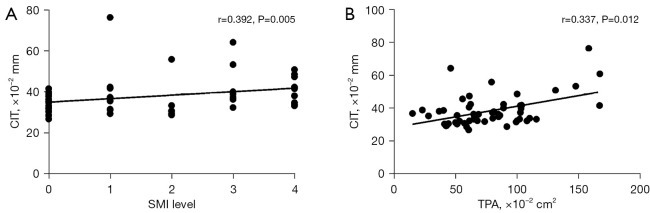
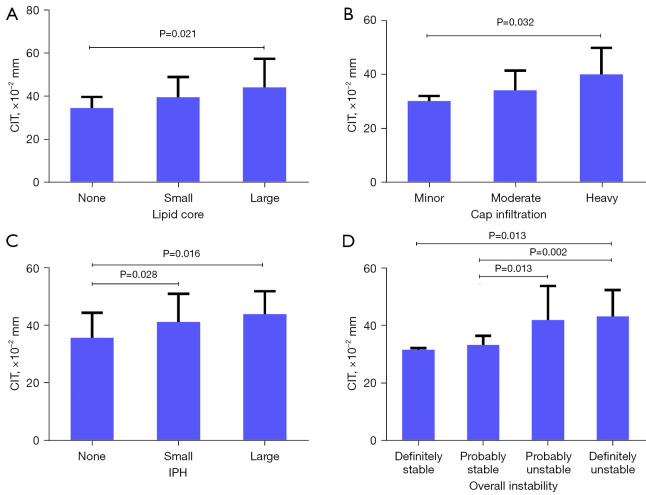
The mean CIT of all the participants was 0.382±0.095 mm, the mean CIT of the participants with stable plaques was 0.328±0.031 mm, and the mean CIT of participants with vulnerable plaques was 0.424±0.106 mm (P<0.001). CIT was associated with the SMI level (Spearman's correlation coefficient: r=0.392, P=0.005), TPA (Spearman's correlation coefficient: r=0.337, P=0.012). Patients with thicker CIT had larger lipid cores, higher levels of plaque vulnerability, and more intraplaque hemorrhages (IPHs). The areas under the ROCs (AUCs) with 95% confidence interval (CI) for CIMT, CIT, the SMI level, the GSM, the TPA, and the combined model for identifying vulnerable plaques were 0.673 (0.533-0.793), 0.849 (0.727-0.932), 0.771 (0.629-0.879), 0.669 (0.529-0.790), 0.858 (0.738-0.938), and 0.949 (0.854-0.990), respectively.
CIT was associated with both the histology and ultrasonic features of CP. CIT may be helpful in the detection of severe CP development.
研究表明,颈动脉内膜中层厚度(CIMT)有助于预测轻度颈动脉狭窄患者的颈动脉斑块(CP)进展。然而,关于颈动脉内膜厚度(CIT)在监测重度颈动脉狭窄患者CP发展中的价值,争论仍在继续。本研究旨在评估CIT与CP超声特征之间的关系,并分析CIT和CP超声参数在评估晚期人类颈动脉粥样硬化斑块易损性方面的价值。
本研究共纳入55例行颈动脉内膜切除术(CEA)的个体(平均年龄:65±7岁;女性:9.1%)。在颈总动脉(CCA)处检测CIMT和CIT。还识别了斑块的纹理特征,如灰度中位数(GSM)、超微血管成像(SMI)水平和总斑块面积(TPA)。进行Spearman相关系数分析以检验CIT与CP超声参数之间的关系。比较了不同斑块类型的CIT。采用受试者操作特征(ROC)曲线分析超声特征评估CP易损性的诊断价值。
所有参与者的平均CIT为0.382±0.095mm,稳定斑块参与者的平均CIT为0.328±0.031mm,易损斑块参与者的平均CIT为0.424±0.106mm(P<0.001)。CIT与SMI水平(Spearman相关系数:r=0.392,P=0.005)、TPA(Spearman相关系数:r=0.337,P=0.012)相关。CIT较厚的患者有更大的脂质核心、更高的斑块易损性水平和更多的斑块内出血(IPH)。CIMT、CIT、SMI水平、GSM、TPA以及识别易损斑块的联合模型的ROC曲线下面积(AUC)及其95%置信区间(CI)分别为0.673(0.533-0.793)、0.849(0.727-0.932)、0.771(0.629-0.879)、0.669(0.529-0.790)、0.858(0.738-0.938)和0.949(0.854-0.990)。
CIT与CP的组织学和超声特征均相关。CIT可能有助于检测重度CP的发展。