Lipton Richard B, Schmidt Pete, Diener Hans-Christoph
Albert Einstein College of Medicine, Bronx, NY, USA.
Depomed, Inc, Newark, CA, USA.
Headache. 2017 May;57(5):756-765. doi: 10.1111/head.13073. Epub 2017 Apr 6.
To determine whether baseline nausea or prior triptan treatment for migraine impact the effectiveness of diclofenac potassium for oral solution in treating acute migraine.
A great deal of variability exists in patients' response to migraine medications. Migraine-associated nausea is common and debilitating and can reduce the effectiveness of oral medications. It may cause patients to delay taking oral medications, which is known to diminish therapeutic outcomes, or to avoid taking them altogether. Gastroparesis, which may be associated with nausea, also inhibits drug absorption, resulting in lower bioavailability. Studies have shown that having nausea at the time of drug administration predicts a poorer response to triptan treatment. It is of interest to understand how effective other migraine medications are in patients with a poor response to triptans.
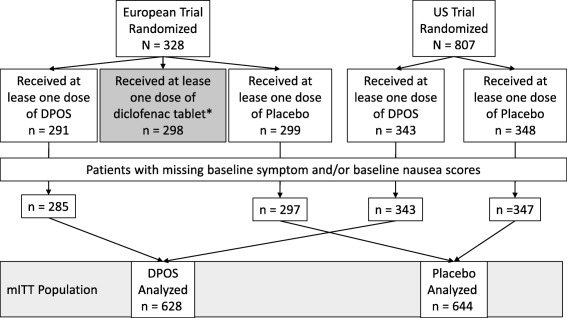
Data from two randomized, double-blind, placebo controlled trials were pooled and post hoc subgroup analyses were performed in patients with and without nausea at baseline, and in patients with and without prior triptan treatment. Efficacy assessments included the percentage of patients who, at 2 hours postdosing, were headache pain-free (2hPF, primary endpoint), without photophobia, without phonophobia, without nausea, or without a severe degree of disability. A Cochran-Mantel-Haenszel test, stratified by analysis center was used to evaluate treatment effect. Effects of nausea or prior triptan use were determined using logistic regression with factors of treatment group, analysis center, nausea or prior triptan use at time of dosing, and interaction of treatment group by nausea or prior triptan use at time of dosing.
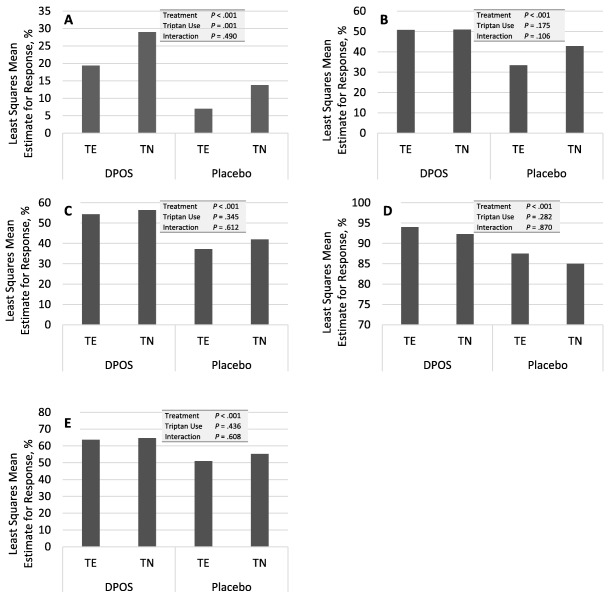
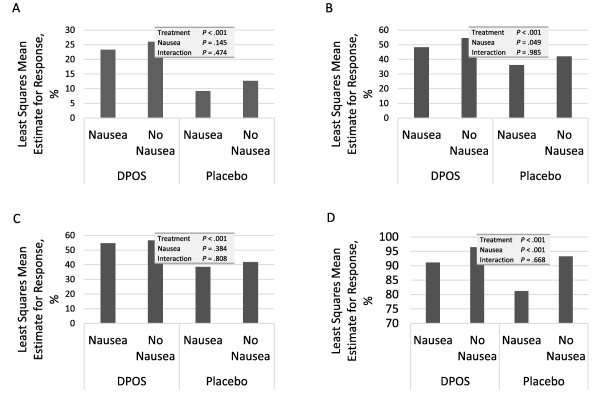
The modified intent to treat population consisted of 1272 patients, 644 on active drug and 628 on placebo. The majority of patients (85%) were female. At the time of dosing, 783 (62%) patients reported nausea with the treated attack. Prior triptan use was recorded in 570 (45%). For headache pain, nausea, photophobia, and phonophobia, patients in the active treatment group had a statistically significantly better response than those receiving placebo, regardless of whether they had nausea at baseline. In logistic regression analysis only treatment group predicted a response for these parameters with no detectable group interaction. Baseline nausea, as well as treatment group, predicted whether patients recorded severe disability at 2 hours. While patients in the active treatment group were significantly more likely to be headache pain-free at 2 hours after dosing, whether or not they had previously been treated with triptan, more triptan-naïve patients (30%) than triptan-experienced patients (20%) were headache pain-free. Interestingly, in the placebo groups, triptan-naïve patients were also more likely to be PF (14% vs 7%). In the logistic regression analysis, treatment group predicted a headache pain response, triptan use predicted a lack of response, and there was no interaction between the two. Prior triptan use did not predict any of the other outcome measures.
Nausea at the time of dosing does not diminish the effectiveness of diclofenac potassium for oral solution. The rapid absorption profile may enhance the effectiveness in patients with nausea. Prior triptan use predicted poorer headache response at 2 hours postdose, suggesting the possibility of a subset of patients who are more likely to be refractory to both triptans and diclofenac. Diclofenac potassium for oral solution is effective in triptan-naïve patients but no reliable inference can be made from this study as to about how to order treatment.
确定偏头痛患者基线时的恶心症状或既往使用曲坦类药物治疗是否会影响口服双氯芬酸钾治疗急性偏头痛的疗效。
患者对偏头痛药物的反应存在很大差异。偏头痛相关的恶心症状常见且使人虚弱,会降低口服药物的疗效。这可能导致患者延迟服用口服药物(已知这会降低治疗效果)或完全避免服用。胃轻瘫可能与恶心有关,也会抑制药物吸收,导致生物利用度降低。研究表明,给药时出现恶心症状预示着对曲坦类药物治疗的反应较差。了解其他偏头痛药物对曲坦类药物反应不佳的患者的疗效如何,很有意义。
汇总两项随机、双盲、安慰剂对照试验的数据,并对基线时有恶心症状和无恶心症状的患者,以及既往有曲坦类药物治疗史和无曲坦类药物治疗史的患者进行事后亚组分析。疗效评估包括给药后2小时头痛缓解(2小时头痛缓解,主要终点)、无畏光、无畏声、无恶心或无严重功能障碍的患者百分比。采用按分析中心分层的Cochran-Mantel-Haenszel检验评估治疗效果。使用逻辑回归分析确定恶心或既往使用曲坦类药物的影响,分析因素包括治疗组、分析中心、给药时的恶心或既往使用曲坦类药物情况,以及治疗组与给药时恶心或既往使用曲坦类药物情况的交互作用。
改良意向性治疗人群包括1272例患者,644例接受活性药物治疗,628例接受安慰剂治疗。大多数患者(85%)为女性。给药时,783例(62%)患者报告此次发作伴有恶心。570例(45%)患者有既往使用曲坦类药物的记录。对于头痛、恶心、畏光和畏声,活性治疗组的患者在统计学上比接受安慰剂的患者反应更好,无论他们基线时是否有恶心症状。在逻辑回归分析中,只有治疗组可预测这些参数的反应,未检测到组间交互作用。基线恶心症状以及治疗组可预测患者在2小时时是否有严重功能障碍。虽然活性治疗组的患者在给药后2小时头痛缓解的可能性显著更高,但无论他们之前是否接受过曲坦类药物治疗,未使用过曲坦类药物的患者(30%)比使用过曲坦类药物的患者(20%)头痛缓解的比例更高。有趣的是,在安慰剂组中,未使用过曲坦类药物的患者头痛缓解的可能性也更高(14%对7%)。在逻辑回归分析中,治疗组可预测头痛反应,使用曲坦类药物可预测无反应,两者之间无交互作用。既往使用曲坦类药物不能预测任何其他结局指标。
给药时的恶心症状不会降低口服双氯芬酸钾的疗效。快速吸收特性可能会提高对有恶心症状患者的疗效。既往使用曲坦类药物预示给药后2小时头痛反应较差,提示可能存在一部分对曲坦类药物和双氯芬酸钾均更易产生耐药性的患者。口服双氯芬酸钾对未使用过曲坦类药物的患者有效,但本研究无法就如何安排治疗得出可靠推论。