Sekhon Mypinder S, Ainslie Philip N, Griesdale Donald E
Division of Critical Care Medicine, Department of Medicine, Vancouver General Hospital, University of British Columbia, Room 2438, Jim Pattison Pavilion, 2nd Floor, 855 West 12th Avenue, Vancouver, BC, V5Z 1M9, Canada.
Centre for Heart, Lung and Vascular Health, School of Health and Exercise Sciences, University of British Columbia Okanagan, Kelowna, BC, Canada.
Crit Care. 2017 Apr 13;21(1):90. doi: 10.1186/s13054-017-1670-9.
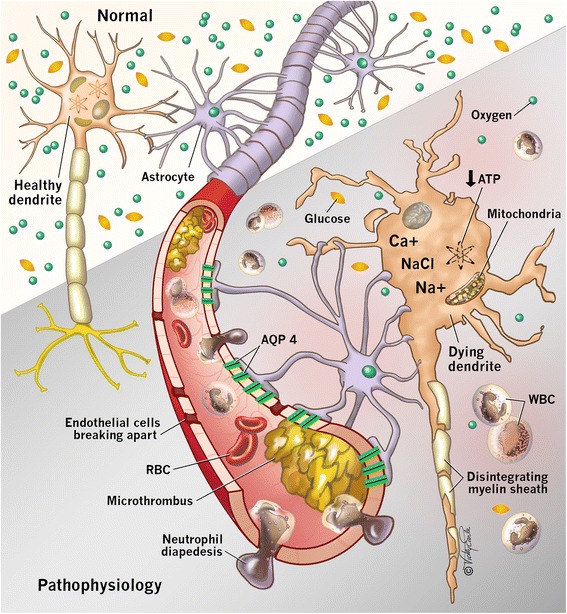
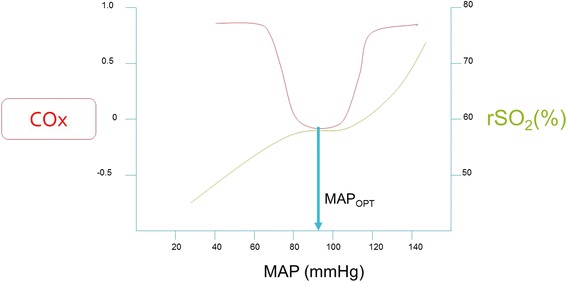
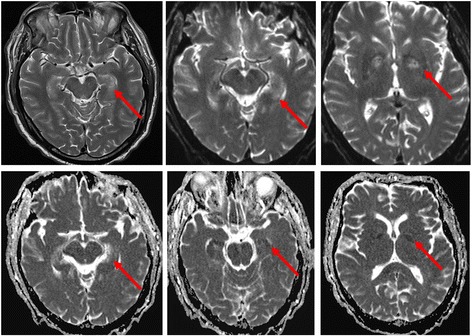
Hypoxic ischemic brain injury (HIBI) after cardiac arrest (CA) is a leading cause of mortality and long-term neurologic disability in survivors. The pathophysiology of HIBI encompasses a heterogeneous cascade that culminates in secondary brain injury and neuronal cell death. This begins with primary injury to the brain caused by the immediate cessation of cerebral blood flow following CA. Thereafter, the secondary injury of HIBI takes place in the hours and days following the initial CA and reperfusion. Among factors that may be implicated in this secondary injury include reperfusion injury, microcirculatory dysfunction, impaired cerebral autoregulation, hypoxemia, hyperoxia, hyperthermia, fluctuations in arterial carbon dioxide, and concomitant anemia.Clarifying the underlying pathophysiology of HIBI is imperative and has been the focus of considerable research to identify therapeutic targets. Most notably, targeted temperature management has been studied rigorously in preventing secondary injury after HIBI and is associated with improved outcome compared with hyperthermia. Recent advances point to important roles of anemia, carbon dioxide perturbations, hypoxemia, hyperoxia, and cerebral edema as contributing to secondary injury after HIBI and adverse outcomes. Furthermore, breakthroughs in the individualization of perfusion targets for patients with HIBI using cerebral autoregulation monitoring represent an attractive area of future work with therapeutic implications.We provide an in-depth review of the pathophysiology of HIBI to critically evaluate current approaches for the early treatment of HIBI secondary to CA. Potential therapeutic targets and future research directions are summarized.
心脏骤停(CA)后的缺氧缺血性脑损伤(HIBI)是幸存者死亡和长期神经功能残疾的主要原因。HIBI的病理生理学包括一个异质性级联反应,最终导致继发性脑损伤和神经元细胞死亡。这始于CA后脑血流立即停止所导致的原发性脑损伤。此后,HIBI的继发性损伤发生在初始CA和再灌注后的数小时和数天内。可能与这种继发性损伤有关的因素包括再灌注损伤、微循环功能障碍、脑自动调节受损、低氧血症、高氧血症、高热、动脉二氧化碳波动以及合并贫血。阐明HIBI的潜在病理生理学至关重要,并且一直是确定治疗靶点的大量研究的重点。最值得注意的是,靶向温度管理已被严格研究用于预防HIBI后的继发性损伤,与高热相比,其与改善预后相关。最近的进展表明,贫血、二氧化碳紊乱、低氧血症、高氧血症和脑水肿在HIBI后的继发性损伤和不良后果中起重要作用。此外,使用脑自动调节监测对HIBI患者进行灌注靶点个体化的突破代表了一个具有治疗意义的未来有吸引力的工作领域。我们对HIBI的病理生理学进行了深入综述,以批判性地评估目前对CA继发的HIBI进行早期治疗的方法。总结了潜在的治疗靶点和未来的研究方向。