Pestalozzi Bernhard C, Tausch Christoph, Dedes Konstantin J, Rochlitz Christoph, Zimmermann Stefan, von Moos Roger, Winterhalder Ralph, Ruhstaller Thomas, Mueller Andreas, Buser Katharina, Borner Markus, Novak Urban, Nussbaum Catrina Uhlmann, Seifert Bettina, Bigler Martin, Bize Vincent, Vilei Simona Berardi, Rageth Christoph, Aebi Stefan
Universitaetsspital Zuerich, Raemistrasse 100, 8091, Zurich, Switzerland.
Brustzentrum Zuerich, Zurich, Switzerland.
BMC Cancer. 2017 Apr 13;17(1):265. doi: 10.1186/s12885-017-3261-1.
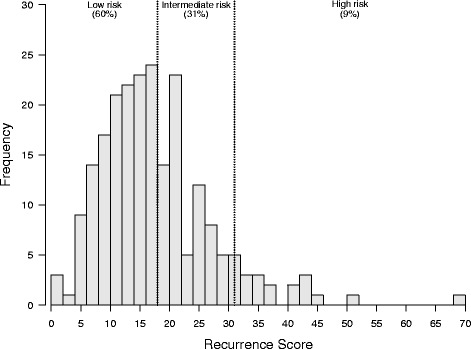
To evaluate the effect of Recurrence Score® results (RS; Oncotype DX® multigene assay ODX) on treatment recommendations by Swiss multidisciplinary tumor boards (TB).
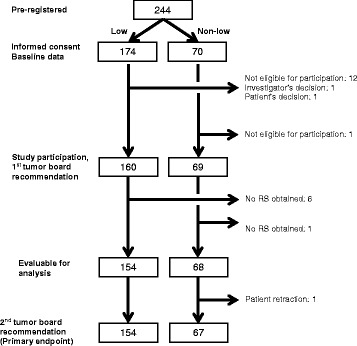
SAKK 26/10 is a multicenter, prospective cohort study of early breast cancer patients: Eligibility: R0-resection, ≥10% ER+ malignant cells, HER2-, pN0/pN1a. Patients were stratified into low-risk (LR) and non-low-risk (NLR) groups based on involved nodes (0 vs 1-3) and five additional predefined risk factors. Recommendations were classified as hormonal therapy (HT) or chemotherapy plus HT (CT + HT). Investigators were blinded to the statistical analysis plan. A 5%/10% rate of recommendation change in LR/NLR groups, respectively, was assumed independently of RS (null hypotheses).
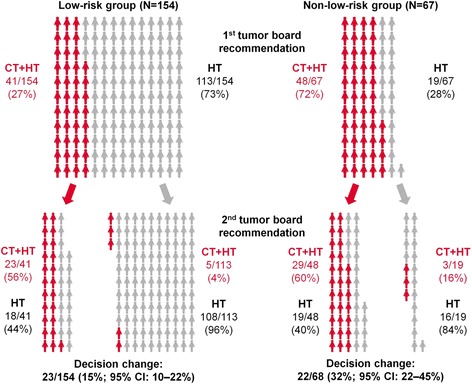
Two hundred twenty two evaluable patients from 18 centers had TB recommendations before and after consideration of the RS result. A recommendation change occurred in 45 patients (23/154 (15%, 95% CI 10-22%) in the LR group and 22/68 (32%, 95% CI 22-45%) in the NLR group). In both groups the null hypothesis could be rejected (both p < 0.001). Specifically, in the LR group, only 5/113 (4%, 95% CI 1-10%) with HT had a recommendation change to CT + HT after consideration of the RS, while 18/41 (44%, 95% CI 28-60%) of patients initially recommended CT + HT were subsequently recommended only HT. In the NLR group, 3/19 (16%, 95% CI 3-40%) patients were changed from HT to CT + HT, while 19/48 (40%, 95% CI 26-55%) were changed from CT + HT to HT.
There was a significant impact of using the RS in the LR and the NLR group but only 4% of LR patients initially considered for HT had a recommendation change (RC); therefore these patients could forgo ODX testing. A RC was more likely for NLR patients considered for HT. Patients considered for HT + CT have the highest likelihood of a RC based on RS.
评估复发评分(RS;Oncotype DX多基因检测ODX)结果对瑞士多学科肿瘤委员会(TB)治疗建议的影响。
SAKK 26/10是一项针对早期乳腺癌患者的多中心前瞻性队列研究:入选标准:R0切除、ER+恶性细胞≥10%、HER2阴性、pN0/pN1a。根据受累淋巴结情况(0个 vs 1 - 3个)及另外五个预先定义的风险因素,将患者分为低风险(LR)组和非低风险(NLR)组。建议分为激素治疗(HT)或化疗加激素治疗(CT + HT)。研究人员对统计分析计划不知情。分别假设LR/NLR组中建议改变率为5%/10%,与RS无关(零假设)。
来自18个中心的222例可评估患者在考虑RS结果前后有TB给出的建议。45例患者的建议发生了改变(LR组中23/154例(15%,95%置信区间10 - 22%),NLR组中22/68例(32%,95%置信区间22 - 45%))。两组的零假设均被拒绝(均p < 0.001)。具体而言,在LR组中,最初接受HT的患者中只有5/113例(4%,95%置信区间1 - 10%)在考虑RS后建议改为CT + HT,而最初建议CT + HT的患者中有18/41例(44%,95%置信区间28 - 60%)随后仅被建议接受HT。在NLR组中,3/19例(16%,95%置信区间3 - 40%)患者从HT改为CT + HT,而19/48例(40%,95%置信区间26 - 55%)从CT + HT改为HT。
在LR组和NLR组中使用RS有显著影响,但最初考虑接受HT的LR患者中只有4%的建议发生了改变(RC);因此这些患者可以不进行ODX检测。考虑接受HT的NLR患者更有可能发生RC。考虑接受HT + CT的患者基于RS发生RC的可能性最高。