Foot Holly, Freeman Christopher, Hemming Karla, Scott Ian, Coombes Ian D, Williams Ian D, Connelly Luke, Whitty Jennifer A, Sturman Nancy, Kirsa Sue, Nicholson Caroline, Russell Grant, Kirkpatrick Carl, Cottrell Neil
School of Pharmacy, University of Queensland, Brisbane, Queensland, Australia.
School of Pharmacy, University of Queensland, Brisbane, Queensland, Australia
BMJ Open. 2017 Apr 13;7(4):e015301. doi: 10.1136/bmjopen-2016-015301.
A model of general practitioner (GP) and pharmacist collaboration in primary care may be an effective strategy to reduce medication-related problems and provide better support to patients after discharge. The aim of this study is to investigate whether a model of structured pharmacist and GP care reduces hospital readmissions in high-risk patients.
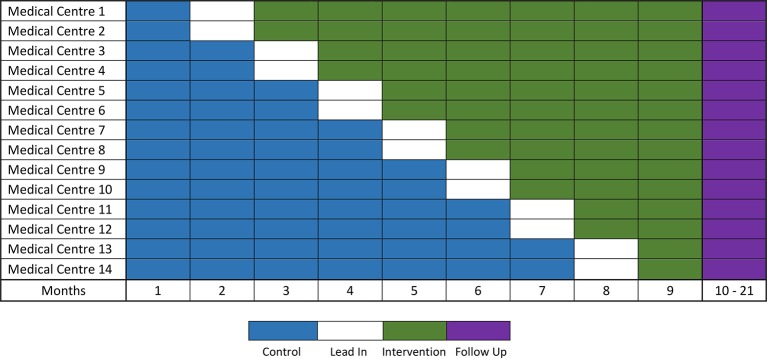
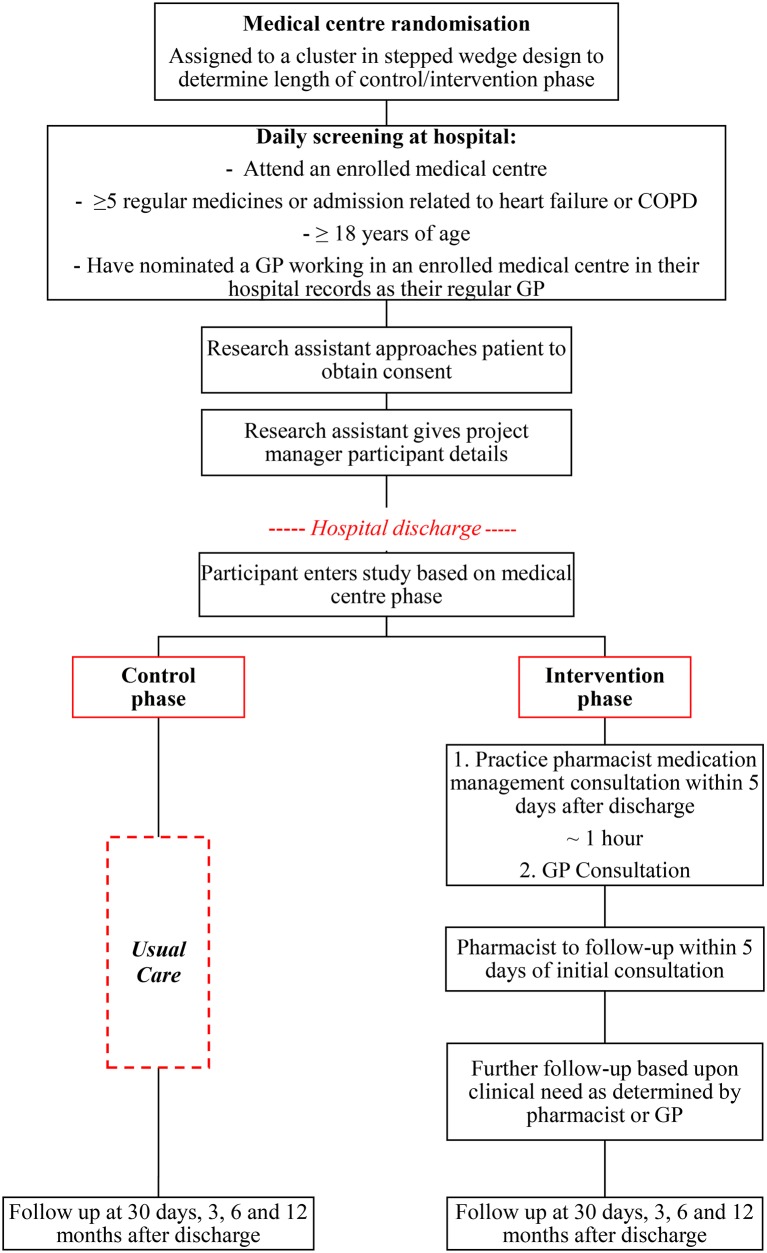
This protocol details a stepped-wedge, cluster-randomised trial that will recruit participants over 9 months with a 12-month follow-up. There will be 14 clusters each representing a different general practice medical centre. A total of 2240 participants will be recruited from hospital who attend an enrolled medical centre, take five or more long-term medicines or whose reason for admission was related to heart failure or chronic obstructive pulmonary disease.The intervention is a multifaceted service, involving a pharmacist integrated into a medical centre to assist patients after hospitalisation. Participants will meet with the practice pharmacist and their GP after discharge to review and reconcile their medicines and discuss changes made in hospital. The pharmacist will follow-up with the participant and liaise with other health professionals involved in the participant's care. The control will be usual care, which usually involves a patient self-organising a visit to their GP after hospital discharge.The primary outcome is the rate of unplanned, all-cause hospital readmissions over 12 months, which will be analysed using a mixed effects Poisson regression model with a random effect for cluster and a fixed effect to account for any temporal trend. A cost analysis will be undertaken to compare the healthcare costs associated with the intervention to those of usual care.
The study has received ethical approval (HREC/16/QRBW/410). The study findings will be disseminated through peer-reviewed publications, conferences and reports to key stakeholders.
ACTRN12616001627448.
基层医疗中全科医生(GP)与药剂师合作的模式可能是减少药物相关问题并在患者出院后提供更好支持的有效策略。本研究的目的是调查结构化药剂师与全科医生护理模式是否能降低高危患者的医院再入院率。
本方案详细介绍了一项阶梯楔形整群随机试验,该试验将在9个月内招募参与者,并进行12个月的随访。共有14个整群,每个整群代表一个不同的全科医疗中心。将从医院招募总共2240名参与者,这些参与者需在注册医疗中心就诊、服用五种或更多长期药物,或者入院原因与心力衰竭或慢性阻塞性肺疾病相关。干预措施是一项多方面的服务,包括一名药剂师融入医疗中心以在患者出院后提供协助。参与者出院后将与执业药剂师及其全科医生会面,以审查和核对他们的药物,并讨论在医院所做的更改。药剂师将对参与者进行随访,并与参与该参与者护理的其他医疗专业人员进行联络。对照组为常规护理,通常包括患者出院后自行安排就诊全科医生。主要结局是12个月内非计划的全因医院再入院率,将使用混合效应泊松回归模型进行分析,该模型具有整群的随机效应和用于解释任何时间趋势的固定效应。将进行成本分析,以比较干预措施与常规护理相关的医疗保健成本。
本研究已获得伦理批准(HREC/16/QRBW/410)。研究结果将通过同行评审的出版物、会议和向主要利益相关者的报告进行传播。
ACTRN12616001627448。