Aberle Teresa, Bourn Rebecka L, Chen Hua, Roberts Virginia C, Guthridge Joel M, Bean Krista, Robertson Julie M, Sivils Kathy L, Rasmussen Astrid, Liles Meghan, Merrill Joan T, Harley John B, Olsen Nancy J, Karp David R, James Judith A
Department of Arthritis and Clinical Immunology, Oklahoma Medical Research Foundation, Oklahoma City, Oklahoma, USA.
Cincinnati Children's Hospital Medical Center and US Department of Veterans Affairs Medical Center, Cincinnati, Ohio, USA.
Lupus Sci Med. 2017 Mar 17;4(1):e000176. doi: 10.1136/lupus-2016-000176. eCollection 2017.
SLE is traditionally classified using the American College of Rheumatology (ACR) criteria. The Systemic Lupus International Collaborating Clinics (SLICC) recently validated an alternative system. This study examined large cohorts of subjects with SLE and incomplete lupus erythematosus (ILE) to compare the impact of ACR and SLICC criteria.
Medical records of subjects in the Lupus Family Registry and Repository were reviewed for documentation of 1997 ACR classification criteria, SLICC classification criteria and medication usage. Autoantibodies were assessed by indirect immunofluorescence (ANA, antidouble-stranded DNA), precipitin (Sm) and ELISA (anticardiolipin). Other relevant autoantibodies were detected by precipitin and with a bead-based multiplex assay.
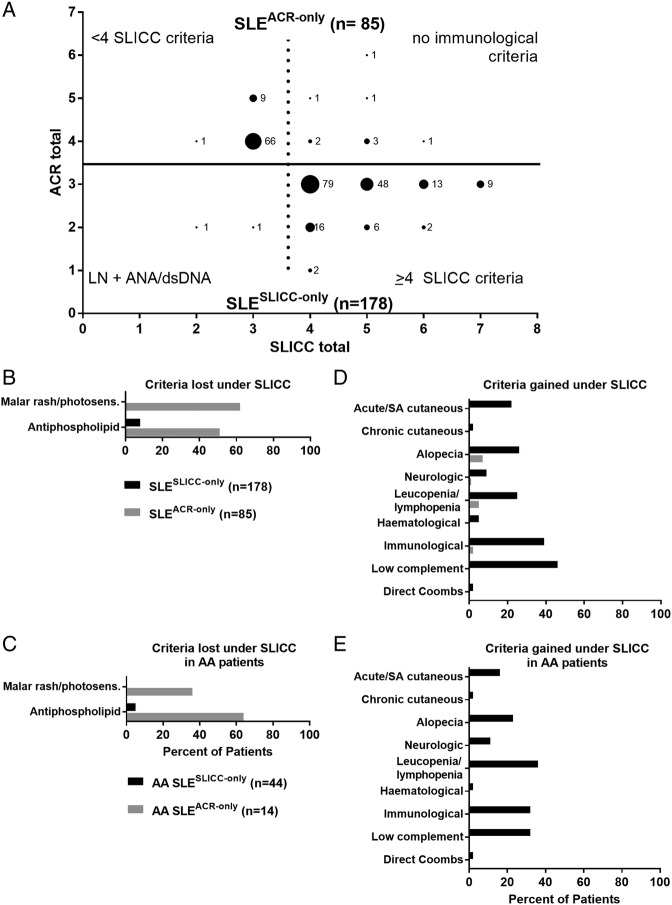
Of 3575 subjects classified with SLE under at least one system, 3312 (92.6%) were classified as SLE by both systems (SLE), 85 only by ACR criteria (SLE) and 178 only by SLICC criteria (SLE). Of 440 subjects meeting 3 ACR criteria, 33.9% (149/440) were SLE, while 66.1% (n=291, designated ILE) did not meet the SLICC classification criteria. Under the SLICC system, the complement criterion and the individual autoantibody criteria enabled SLE classification of SLE subjects, while SLE subjects failed to meet SLICC classification due to the combined acute/subacute cutaneous criterion. The SLICC criteria classified more African-American subjects by the leucopenia/lymphopenia criterion than did ACR criteria. Compared with SLE subjects, SLE subjects exhibited similar numbers of affected organ systems, rates of major organ system involvement (∼30%: pulmonary, cardiovascular, renal, neurological) and medication history.
The SLICC criteria classify more subjects with SLE than ACR criteria; however, individuals with incomplete lupus still exist under SLICC criteria. Subjects who gain SLE classification through SLICC criteria exhibit heterogeneous disease, including potential major organ involvement. These results provide supportive evidence that SLICC criteria may be more inclusive of SLE subjects for clinical studies.
系统性红斑狼疮(SLE)传统上采用美国风湿病学会(ACR)标准进行分类。系统性红斑狼疮国际协作临床中心(SLICC)最近验证了一种替代分类系统。本研究对大量SLE患者和不完全性红斑狼疮(ILE)患者队列进行了检查,以比较ACR和SLICC标准的影响。
回顾狼疮家族登记与资料库中受试者的病历,以记录1997年ACR分类标准、SLICC分类标准及用药情况。通过间接免疫荧光法(抗核抗体、抗双链DNA)、沉淀素法(Sm)和酶联免疫吸附测定法(抗心磷脂)评估自身抗体。其他相关自身抗体通过沉淀素法和基于微珠的多重检测法进行检测。
在至少一种分类系统下被分类为SLE的3575名受试者中,3312名(92.6%)在两种系统下均被分类为SLE,85名仅根据ACR标准被分类为SLE,178名仅根据SLICC标准被分类为SLE。在符合3条ACR标准的440名受试者中,33.9%(149/440)为SLE,而66.1%(n = 291,定为ILE)不符合SLICC分类标准。在SLICC系统下,补体标准和单个自身抗体标准可对SLE患者进行SLE分类,而SLE患者因合并急性/亚急性皮肤标准而未达到SLICC分类标准。与ACR标准相比,SLICC标准通过白细胞减少/淋巴细胞减少标准对更多非裔美国受试者进行了分类。与SLE患者相比,SLE患者受累器官系统数量、主要器官系统受累率(约30%:肺部、心血管、肾脏、神经)及用药史相似。
与ACR标准相比,SLICC标准可对更多SLE患者进行分类;然而,在SLICC标准下仍存在不完全性狼疮患者。通过SLICC标准获得SLE分类的患者表现出异质性疾病,包括潜在的主要器官受累。这些结果提供了支持性证据,表明SLICC标准在临床研究中可能更具包容性。