Tan Yahang, Zhou Jia, Zhou Ying, Yang Xiaobo, Yang Junjie, Chen Yundai
Department of Cardiology, Chinese PLA General Hospital, Beijing 100853, China.
The School of Medicine, Nankai University, Tianjin 300071, China.
Korean J Radiol. 2017 May-Jun;18(3):487-497. doi: 10.3348/kjr.2017.18.3.487. Epub 2017 Apr 3.
This study sought to determine whether variables detected on coronary computed tomography angiography (CCTA) would predict plaque progression in non-culprit lesions (NCL).
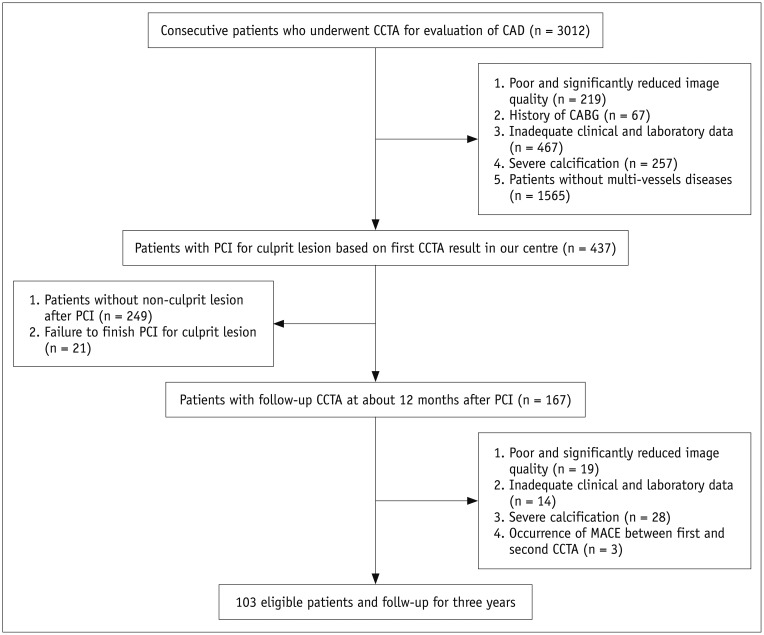
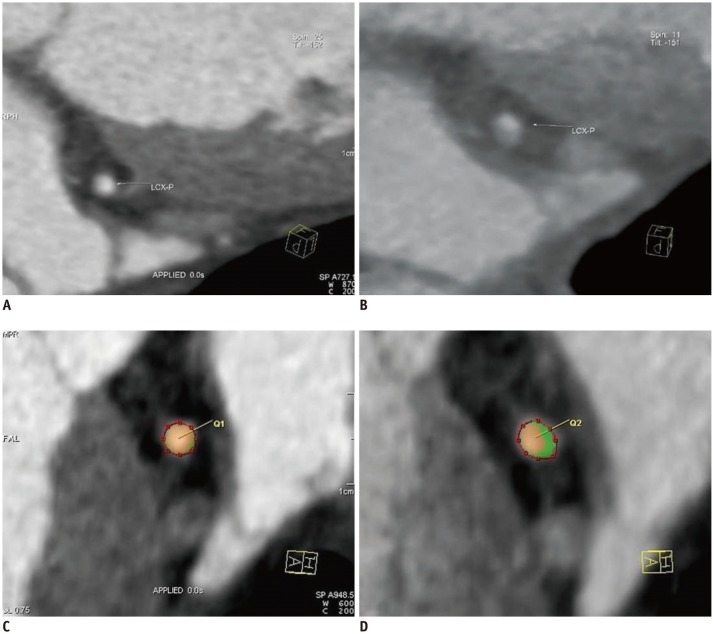
In this single-center trial, we analyzed 103 consecutive patients who were undergoing CCTA and percutaneous coronary intervention (PCI) for culprit lesions. Follow-up CCTA was scheduled 12 months after the PCI, and all patients were followed for 3 years after their second CCTA examination. High-risk plaque features and epicardial adipose tissue (EAT) volume were assessed by CCTA. Each NCL stenosis grade was compared visually between two CCTA scans to detect plaque progression, and patients were stratified into two groups based on this. Logistic regression analysis was used to evaluate the factors that were independently associated with plaque progression in NCLs. Time-to-event curves were compared using the log-rank statistic.
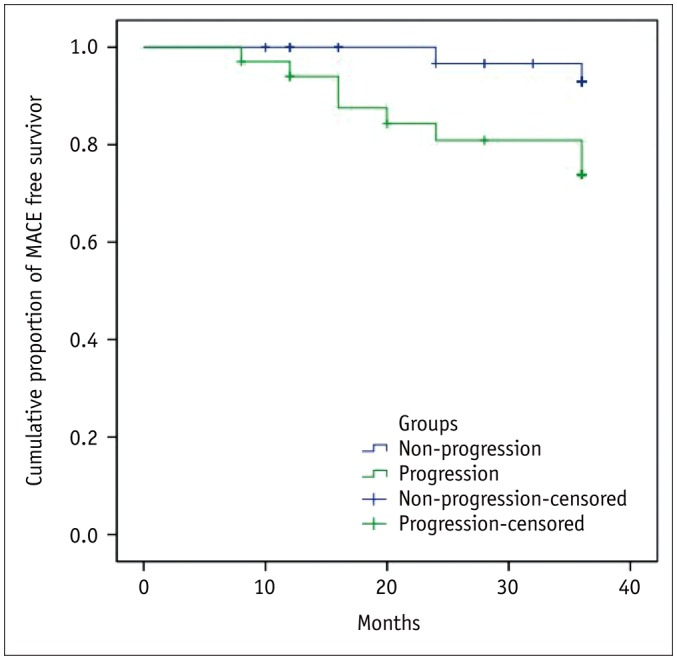
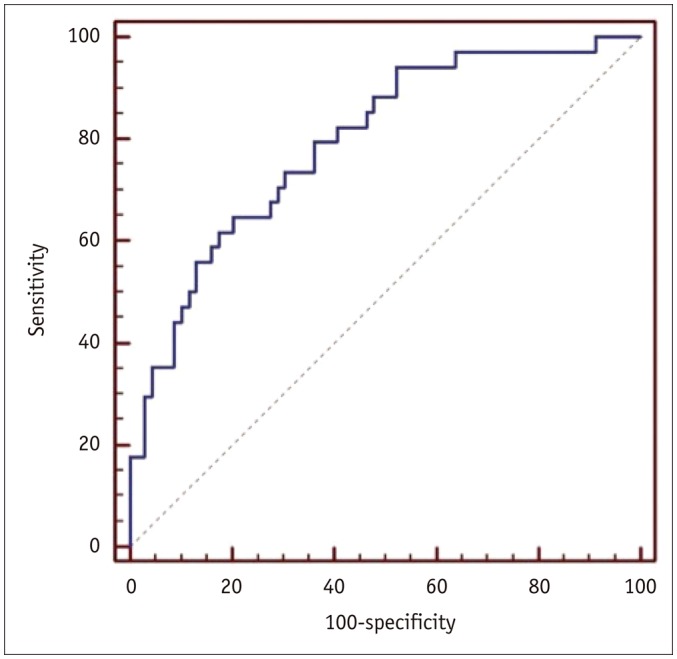
Overall, 34 of 103 patients exhibited NCL plaque progression (33%). Logistic regression analyses showed that the NCL progression was associated with a history of ST-elevated myocardial infarction (odds ratio [OR] = 5.855, 95% confidence interval [CI] = 1.391-24.635, = 0.016), follow-up low-density lipoprotein cholesterol level (OR = 6.832, 95% CI = 2.103-22.200, = 0.001), baseline low-attenuation plaque (OR = 7.311, 95% CI = 1.242-43.028, = 0.028) and EAT (OR = 1.015, 95% CI = 1.000-1.029, = 0.044). Following the second CCTA examination, major adverse cardiac events (MACEs) were observed in 12 patients, and NCL plaque progression was significantly associated with future MACEs (log rank = 0.006).
Noninvasive assessment of NCLs by CCTA has potential prognostic value.
本研究旨在确定冠状动脉计算机断层扫描血管造影(CCTA)检测到的变量是否能预测非罪犯病变(NCL)的斑块进展。
在这项单中心试验中,我们分析了103例因罪犯病变接受CCTA和经皮冠状动脉介入治疗(PCI)的连续患者。PCI术后12个月安排随访CCTA,所有患者在第二次CCTA检查后随访3年。通过CCTA评估高危斑块特征和心外膜脂肪组织(EAT)体积。在两次CCTA扫描之间直观比较每个NCL狭窄程度,以检测斑块进展,并据此将患者分为两组。采用逻辑回归分析评估与NCL斑块进展独立相关的因素。使用对数秩统计量比较事件发生时间曲线。
总体而言,103例患者中有34例出现NCL斑块进展(33%)。逻辑回归分析显示,NCL进展与ST段抬高型心肌梗死病史(比值比[OR]=5.855,95%置信区间[CI]=1.391 - 24.635,P = 0.016)、随访低密度脂蛋白胆固醇水平(OR = 6.832,95%CI = 2.103 - 22.200,P = 0.001)、基线低衰减斑块(OR = 7.311,95%CI = 1.242 - 43.028,P = 0.028)和EAT(OR = 1.015,95%CI = 1.000 - 1.029,P = 0.044)相关。在第二次CCTA检查后,12例患者发生主要不良心脏事件(MACE),NCL斑块进展与未来MACE显著相关(对数秩P = 0.006)。
CCTA对NCL进行无创评估具有潜在的预后价值。