Min Jeong Jin, Cho Hyun Sung, Jeon Suyong, Lee Jong-Hwan, Lee Jeong Jin, Lee Young Tak
Department of Anesthesiology and Pain Medicine Department of Thoracic and Cardiovascular Surgery, Cardiac and Vascular Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea.
Medicine (Baltimore). 2017 May;96(18):e6801. doi: 10.1097/MD.0000000000006801.
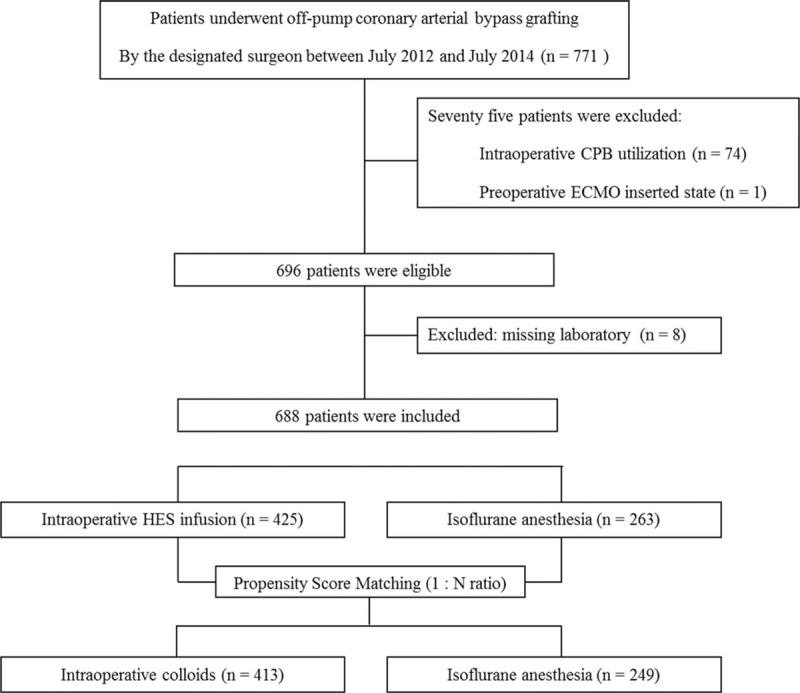
We retrospectively evaluated the effects of 6% hydroxyethyl starch (HES) 130/0.4 on postoperative blood loss and acute kidney injury (AKI) in patients undergoing off-pump coronary artery bypass grafting (OPCAB).Electronic medical records of 771 patients who underwent OPCAB in our hospital between July 2012 and July 2014 were reviewed, and 249 patients without intraoperative HES-exposure (group NoHES) were matched 1:N with intraoperative HES-exposed 413 patients (group HES) based on propensity score. The effects of intraoperative HES on postoperative cumulative blood loss within the first 24 hours, need for bleeding-related reoperation, and occurrence of postoperative AKI (determined by KDIGO and RIFLE criteria) were analyzed.In our propensity score matched cohort, there were no significant differences between groups for median postoperative 24 hours blood loss (525 mL in group HES vs. 540 mL in group NoHES, P = .203) or need for bleeding-related reoperation (OR, 2.44; 95% confidence interval [CI], 0.64-9.34, P = .19). However, postoperative AKI (assessed by 2 criteria) occurred more frequently in group HES than in group NoHES (by KDIGO criteria: 10.7% vs. 3.6%; OR 3.43 [95% CI, 1.67-7.04]; P < .001 and by RIFLE criteria: 9.6% vs. 2%; OR 3.32 [95% CI, 1.34-8.24]; P = .01). The median volume of infused HES per patient weight was 16 mL/kg in group HES.In the patients undergoing OPCAB, intraoperative 6% HES 130/0.4 did not increase postoperative bleeding. However, renal safety remains a concern. Intraoperative use of HES should be determined cautiously during OPCAB.
我们回顾性评估了6%羟乙基淀粉(HES)130/0.4对非体外循环冠状动脉旁路移植术(OPCAB)患者术后失血及急性肾损伤(AKI)的影响。回顾了2012年7月至2014年7月间在我院接受OPCAB的771例患者的电子病历,并根据倾向评分将249例术中未暴露于HES的患者(非HES组)与413例术中暴露于HES的患者(HES组)进行1:N匹配。分析了术中使用HES对术后24小时内累积失血量、出血相关再次手术需求及术后AKI发生情况(根据KDIGO和RIFLE标准判定)的影响。在我们的倾向评分匹配队列中,两组术后24小时中位失血量(HES组525 mL vs.非HES组540 mL,P = 0.203)或出血相关再次手术需求(OR,2.44;95%置信区间[CI],0.64 - 9.34,P = 0.19)无显著差异。然而,HES组术后AKI(根据2项标准评估)的发生率高于非HES组(根据KDIGO标准:10.7% vs. 3.6%;OR 3.43 [95% CI,1.67 - 7.04];P < 0.001,根据RIFLE标准:9.6% vs. 2%;OR 3.32 [95% CI,1.34 - 8.24];P = 0.01)。HES组每位患者体重输注HES的中位体积为16 mL/kg。在接受OPCAB的患者中,术中使用6% HES 130/0.4未增加术后出血。然而,肾脏安全性仍令人担忧。在OPCAB期间,术中使用HES应谨慎决定。