Chen Yu-Jen, Sung Shih-Hsien, Cheng Hao-Min, Huang Wei-Ming, Wu Chung-Li, Huang Chi-Jung, Hsu Pai-Feng, Yeh Jong-Shiuan, Guo Chao-Yu, Yu Wen-Chung, Chen Chen-Huan
Division of Cardiovascular Medicine, Department of Internal Medicine, Wanfang Hospital, Taipei Medical University, Taipei, Taiwan.
Department of Internal Medicine, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan.
J Am Heart Assoc. 2017 May 4;6(5):e004297. doi: 10.1161/JAHA.116.004297.
AHEAD (A: atrial fibrillation; H: hemoglobin; E: elderly; A: abnormal renal parameters; D: diabetes mellitus) score has been related to clinical outcomes of acute heart failure. However, the prognostic value of the AHEAD score in acute heart failure patients with either reduced or preserved left ventricular ejection fraction (HFrEF and HFpEF) remain to be elucidated.
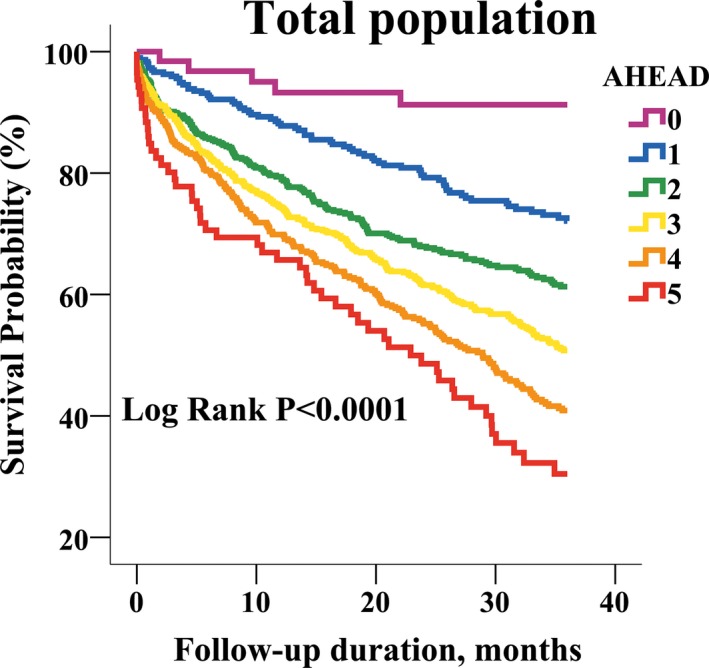
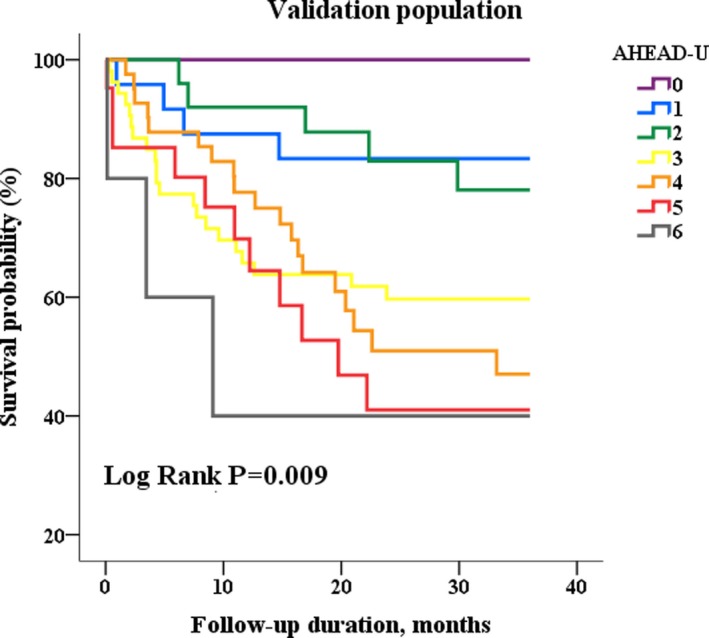
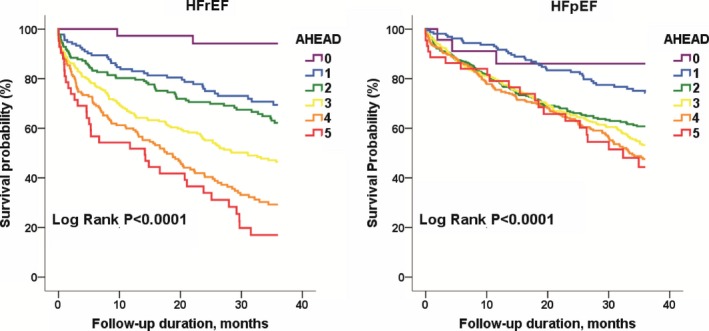
The study population consisted of 2143 patients (age 77±12 years, 68% men, 38% HFrEF) hospitalized primarily for acute heart failure with a median follow-up of 23.75 months. The performance of the AHEAD score (atrial fibrillation, hemoglobin <13 mg/dL for men and 12 mg/dL for women, age >70 years, creatinine >130 μmol/L, and diabetes mellitus) was evaluated by Cox's regression analysis for predicting cardiovascular and all-cause mortality. The mean AHEAD scores were 2.7±1.2 in the total study population, 2.6±1.3 in the HFrEF group, and 2.7±1.1 in the HFpEF group. After accounting for sex, sodium, uric acid, and medications, the AHEAD score remained significantly associated with all-cause and cardiovascular mortality (hazard ratio and 95% CI: 1.49, 1.38-1.60 and 1.48, 1.33-1.64), respectively. The associations of AHEAD score with mortality remained significant in the subgroups of HFrEF (1.63, 1.47-1.82) and HFpEF (1.34, 1.22-1.48). Moreover, when we calculated a new AHEAD-U score by considering uric acid (>8.6 mg/dL) in addition to the AHEAD score, the net reclassification was improved by 19.7% and 20.1% for predicting all-cause and cardiovascular mortality, respectively.
The AHEAD score was useful in predicting long-term mortality in the Asian acute heart failure cohort with either HFrEF or HFpEF. The new AHEAD-U score may further improve risk stratification.
AHEAD(A:心房颤动;H:血红蛋白;E:老年;A:肾功能异常;D:糖尿病)评分与急性心力衰竭的临床结局相关。然而,AHEAD评分在左心室射血分数降低或保留的急性心力衰竭患者(射血分数降低的心力衰竭和射血分数保留的心力衰竭)中的预后价值仍有待阐明。
研究人群包括2143例患者(年龄77±12岁,68%为男性,38%为射血分数降低的心力衰竭患者),主要因急性心力衰竭住院,中位随访时间为23.75个月。通过Cox回归分析评估AHEAD评分(心房颤动、男性血红蛋白<13mg/dL、女性血红蛋白<12mg/dL、年龄>70岁、肌酐>130μmol/L和糖尿病)对心血管和全因死亡率的预测性能。在整个研究人群中,AHEAD评分的平均值为2.7±1.2,在射血分数降低的心力衰竭组中为2.6±1.3,在射血分数保留的心力衰竭组中为2.7±1.1。在考虑性别、钠、尿酸和药物因素后,AHEAD评分仍与全因死亡率和心血管死亡率显著相关(风险比和95%可信区间分别为:1.49,1.38 - 1.60和1.48,1.33 - 1.64)。AHEAD评分与死亡率的关联在射血分数降低的心力衰竭亚组(1.63,1.47 - 1.82)和射血分数保留的心力衰竭亚组(1.34,1.22 - 1.48)中仍然显著。此外,当我们在AHEAD评分的基础上考虑尿酸(>8.6mg/dL)计算新的AHEAD-U评分时,预测全因死亡率和心血管死亡率的净重新分类分别提高了19.7%和20.1%。
AHEAD评分有助于预测亚洲射血分数降低或保留的急性心力衰竭队列中的长期死亡率。新的AHEAD-U评分可能进一步改善风险分层。