Kalmanovich Eran, Blatt Alex, Brener Svetlana, Shlezinger Meital, Shlomo Nir, Vered Zvi, Hod Hanoch, Goldenberg Ilan, Elbaz-Greener Gabby
Department of Cardiology, Assaf Harofeh Medical Center, Sackler Faculty of Medicine, Tel Aviv University, Zerifin, Israel.
The Heart Center, Chaim Sheba Medical Center, Tel Hashomer, Sackler Faculty of Medicine, Tel Aviv University, Israel.
Oncotarget. 2017 Jun 27;8(26):42876-42886. doi: 10.18632/oncotarget.17152.
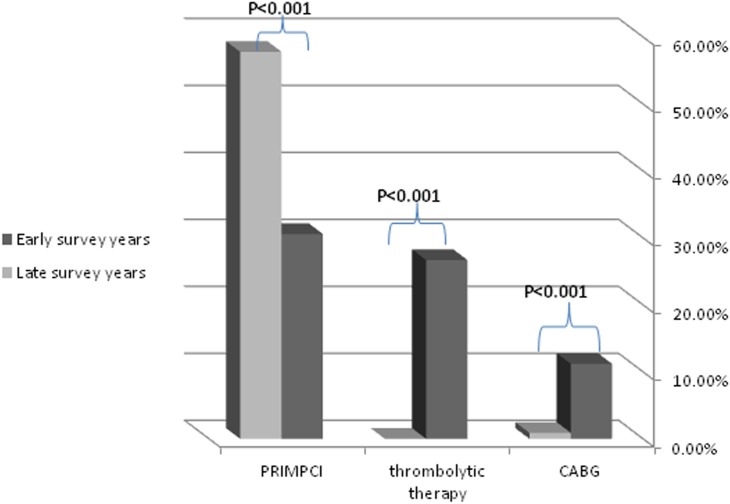
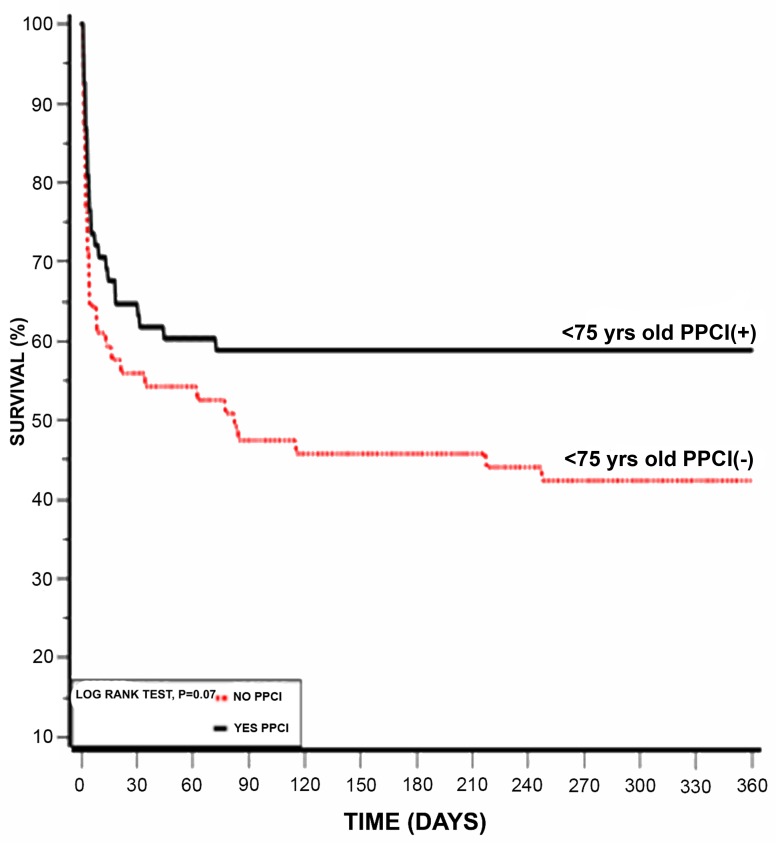
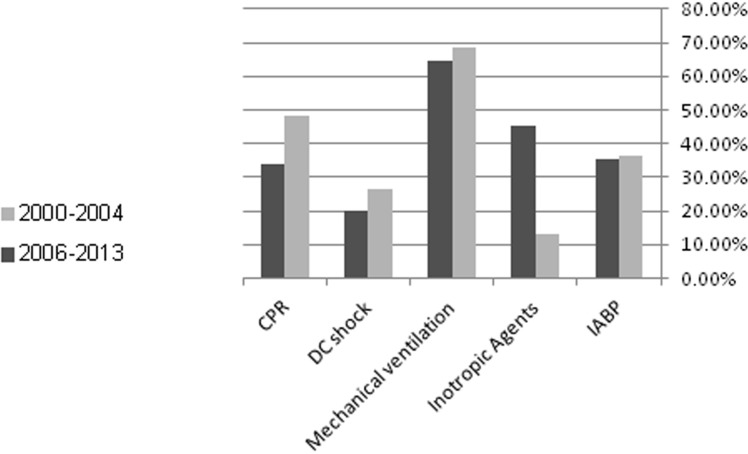
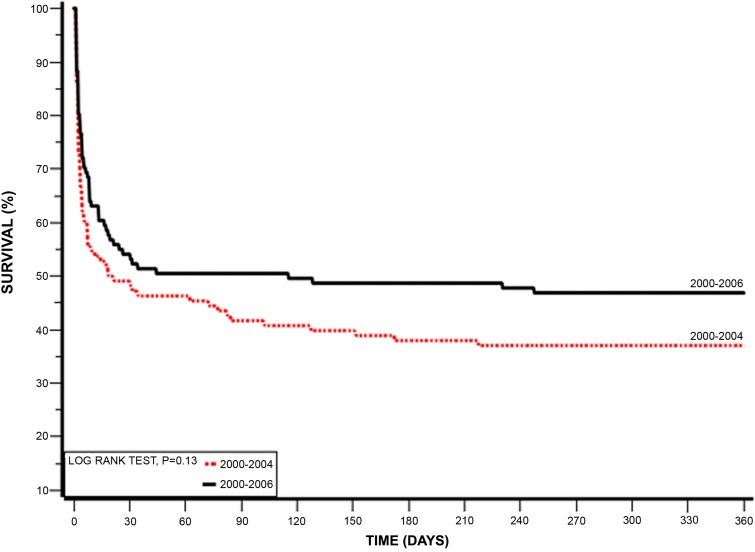
Registries and other cohorts have demonstrated that early revascularization improve the survival of patients presenting with Cardiogenic Shock (CS) completing Aute coronary syndrome (ACS). Our aim was to describe the change in the clinical characteristics of these patients and their management and their outcome. The study population comprised 224 patients who were admitted with ACS complicated by cardiogenic shock who were enrolled in the prospective biannual Acute Coronary Syndrome Israeli Surveys (ACSIS) between 2000 and 2013 (1.7% of all patients admitted with ACS during the study period). Survey periods were categorized as early (years 2000-2004) and late (year 2006-2013).The rate of cardiogenic shock complicated ACS declined from 1.8% between the years 2000-2004 to 1.5% during the years 2006-2013. The clinical presentation in both the early and late groups was similar. During the index hospitalization primary percutaneous coronary intervention (PPCI) was more frequently employed during the late surveys [31% vs. 58% (p<0.001)], while fibrinolysis therapy was not used in the late surveys group [27% vs. 0.0% (p=<0.001)]. Compared to patients enrolled in the early surveys, those enrolled in the late survey group experienced significantly lower mortality rates at 7-days (44% vs. 30%, respectively; p=0.03). However, this difference was no longer statistically significant at 30-days (52.8% vs. 46.4%, respectively, p=0.34) and 1-year (63% vs. 53.2%, respectively, p=0.14). Similarly, the rate of major adverse cardiac events (MACE) at 30-days was similar between the two groups (57.4% vs. 47.4%, respectively, p=0.13).Our findings indicate that patients admitted with ACS complicated by cardiogenic shock still experience very high rates of MACE and mortality during follow-up, despite a significant increase in the use of PPCI in this population over the past decade.
登记处和其他队列研究表明,早期血运重建可提高心源性休克(CS)合并急性冠状动脉综合征(ACS)患者的生存率。我们的目的是描述这些患者的临床特征变化、治疗情况及其预后。研究人群包括224例因ACS并发心源性休克而入院的患者,他们在2000年至2013年期间被纳入前瞻性的以色列急性冠状动脉综合征两年一次调查(ACSIS)(占研究期间所有因ACS入院患者的1.7%)。调查期分为早期(2000 - 2004年)和晚期(2006 - 2013年)。心源性休克合并ACS的发生率从2000 - 2004年的1.8%下降至2006 - 2013年的1.5%。早期和晚期组的临床表现相似。在首次住院期间,晚期调查中更频繁地采用了直接经皮冠状动脉介入治疗(PPCI)[31%对58%(p<0.001)],而晚期调查组未使用溶栓治疗[27%对0.0%(p=<0.001)]。与早期调查纳入的患者相比,晚期调查组的患者在7天时死亡率显著更低(分别为44%对30%;p = 0.03)。然而,在30天时(分别为52.8%对46.4%,p = 0.34)和1年时(分别为63%对53.2%,p = 0.14),这种差异不再具有统计学意义。同样,两组在30天时的主要不良心脏事件(MACE)发生率相似(分别为57.4%对47.4%,p = 0.13)。我们的研究结果表明,尽管在过去十年中该人群使用PPCI的比例显著增加,但因ACS并发心源性休克入院的患者在随访期间仍经历非常高的MACE发生率和死亡率。