McCluskey Suzanne M, Schuetz Philipp, Abers Michael S, Bearnot Benjamin, Morales Maria E, Hoffman Debora, Patel Shreya, Rosario Lauren, Chiappa Victor, Parry Blair A, Callahan Ryan T, Bond Sheila A, Lewandrowski Kent, Binder William, Filbin Michael R, Vyas Jatin M, Mansour Michael K
Department of Medicine, Division of Infectious Diseases, Massachusetts General Hospital, Boston, Massachusetts.
University of Basel, Kantonsspital Aarau, Switzerland; Departments of.
Open Forum Infect Dis. 2017 Jan 4;4(1):ofw238. doi: 10.1093/ofid/ofw238. eCollection 2017 Winter.
Procalcitonin (PCT) is a prohormone that rises in bacterial pneumonia and has promise in reducing antibiotic use. Despite these attributes, there are inconclusive data on its use for clinical prognostication. We hypothesize that serial PCT measurements can predict mortality, intensive care unit (ICU) admission, and bacteremia.
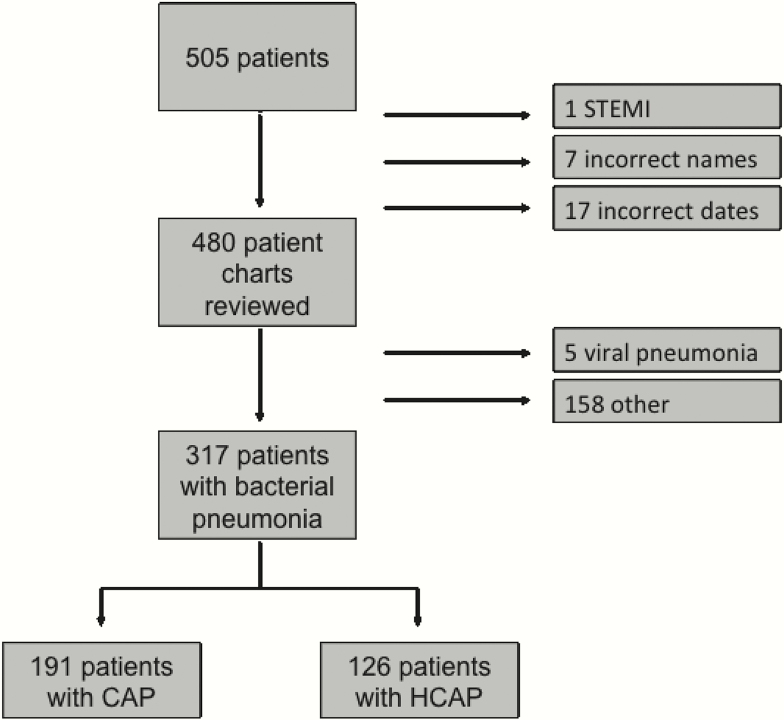
A prospective cohort study of inpatients diagnosed with pneumonia was performed at a large tertiary care center in Boston, Massachusetts. Procalcitonin was measured on days 1 through 4. The primary endpoint was a composite adverse outcome defined as all-cause mortality, ICU admission, and bacteremia. Regression models were calculated with area under the receiver operating characteristic curve (AUC) as a measure of discrimination.
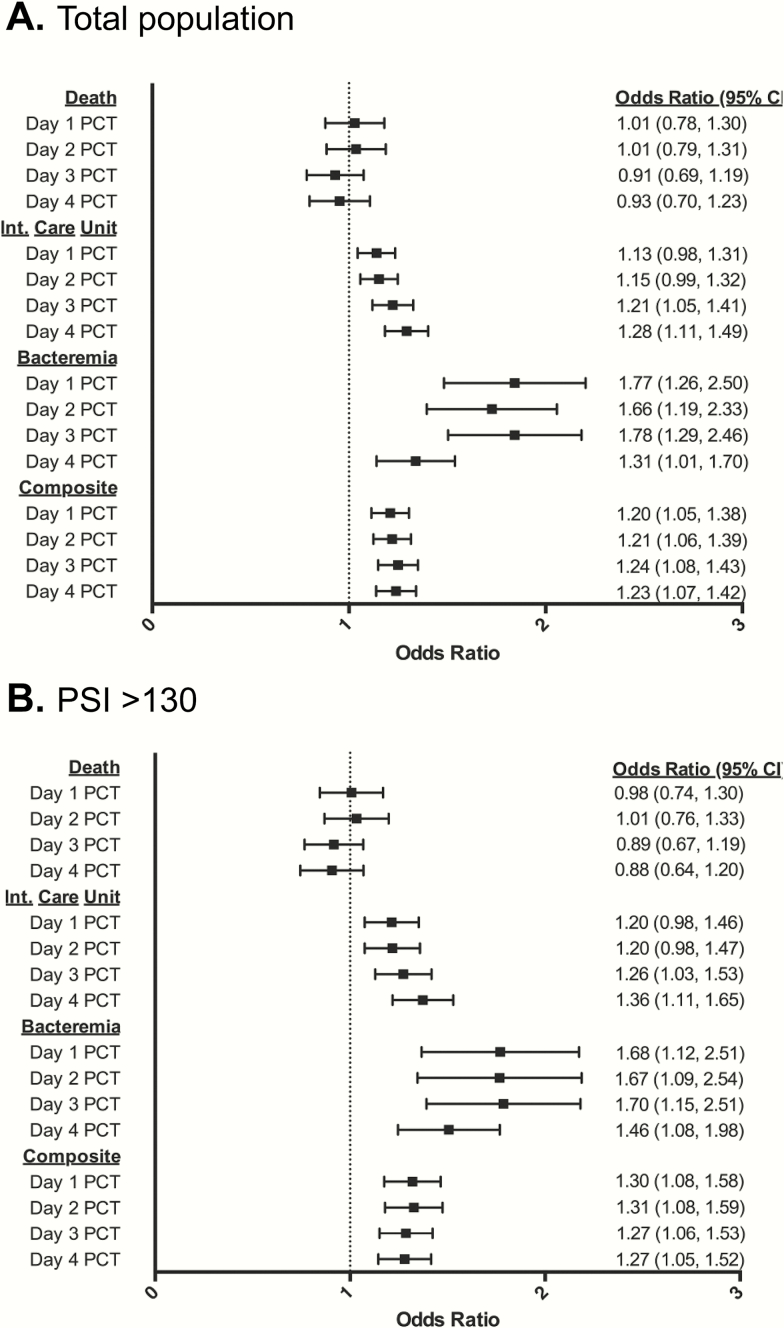
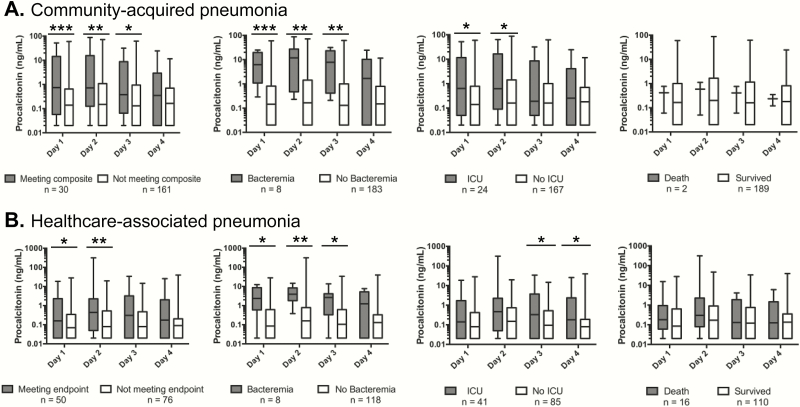
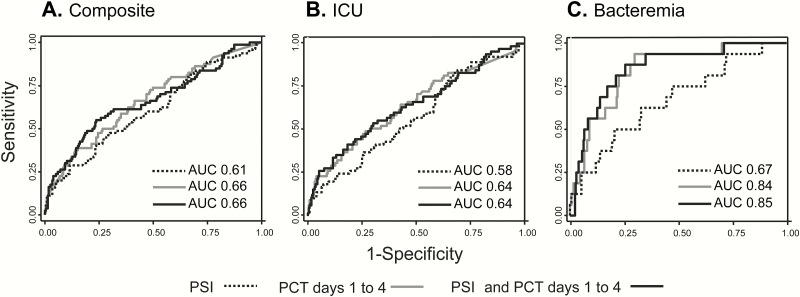
Of 505 patients, 317 patients had a final diagnosis of community-acquired pneumonia (CAP) or healthcare-associated pneumonia (HCAP). Procalcitonin was significantly higher for CAP and HCAP patients meeting the composite primary endpoint, bacteremia, and ICU admission, but not mortality. Incorporation of serial PCT levels into a statistical model including the Pneumonia Severity Index (PSI) improved the prognostic performance of the PSI with respect to the primary composite endpoint (AUC from 0.61 to 0.66), bacteremia (AUC from 0.67 to 0.85), and need for ICU-level care (AUC from 0.58 to 0.64). For patients in the highest risk class PSI >130, PCT was capable of further risk stratification for prediction of adverse outcomes.
Serial PCT measurement in patients with pneumonia shows promise for predicting adverse clinical outcomes, including in those at highest mortality risk.
降钙素原(PCT)是一种前激素,在细菌性肺炎时会升高,有望减少抗生素的使用。尽管有这些特性,但关于其用于临床预后评估的数据尚无定论。我们假设连续测量PCT可以预测死亡率、重症监护病房(ICU)入住率和菌血症。
在马萨诸塞州波士顿的一家大型三级医疗中心对诊断为肺炎的住院患者进行了一项前瞻性队列研究。在第1至4天测量降钙素原。主要终点是一个综合不良结局,定义为全因死亡率、ICU入住率和菌血症。计算回归模型,以受试者操作特征曲线下面积(AUC)作为区分度的指标。
在505例患者中,317例最终诊断为社区获得性肺炎(CAP)或医疗保健相关肺炎(HCAP)。符合综合主要终点、菌血症和ICU入住标准的CAP和HCAP患者的降钙素原水平显著更高,但与死亡率无关。将连续的PCT水平纳入包括肺炎严重程度指数(PSI)的统计模型中,可改善PSI对主要综合终点(AUC从0.61提高到0.66)、菌血症(AUC从0.67提高到0.85)以及ICU级护理需求(AUC从0.58提高到0.64)的预后评估性能。对于PSI>130的最高风险类别患者,PCT能够进一步进行风险分层以预测不良结局。
对肺炎患者连续测量PCT显示出预测不良临床结局的前景,包括那些死亡风险最高的患者。