Capper David, von Deimling Andreas, Brandes Alba A, Carpentier Antoine F, Kesari Santosh, Sepulveda-Sanchez Juan M, Wheeler Helen R, Chinot Olivier, Cher Lawrence, Steinbach Joachim P, Specenier Pol, Rodon Jordi, Cleverly Ann, Smith Claire, Gueorguieva Ivelina, Miles Colin, Guba Susan C, Desaiah Durisala, Estrem Shawn T, Lahn Michael M, Wick Wolfgang
Department of Neuropathology, Charité Universitätsmedizin Berlin, Charitéplatz 1, 10117 Berlin, Germany.
Department of Neuropathology, University Hospital Heidelberg and Clinical Cooperation Unit Neuropathology, German Cancer Consortium (DKTK), German Cancer Research Center (DKFZ), 69120 Heidelberg, Germany.
Int J Mol Sci. 2017 May 6;18(5):995. doi: 10.3390/ijms18050995.
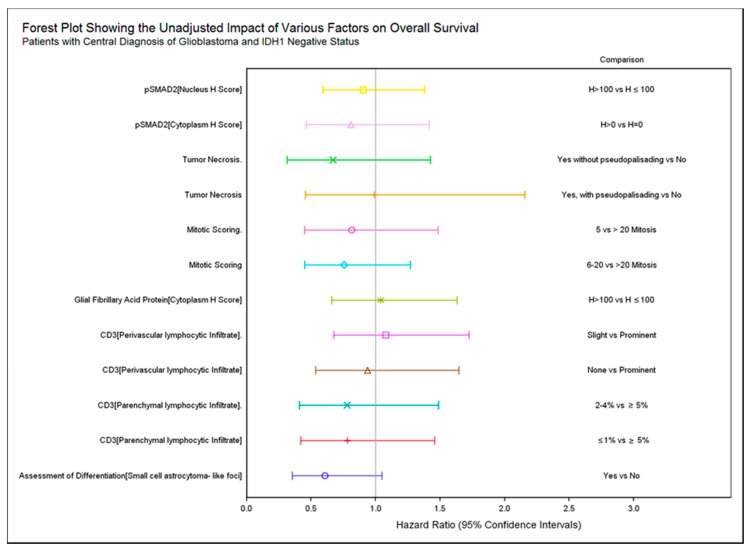
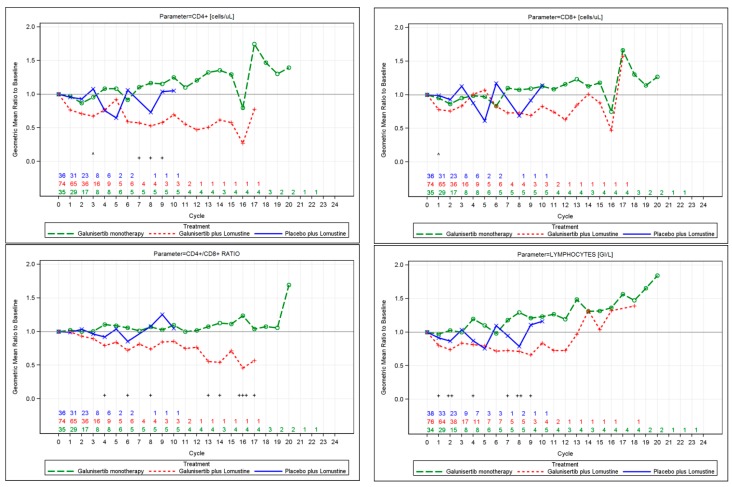
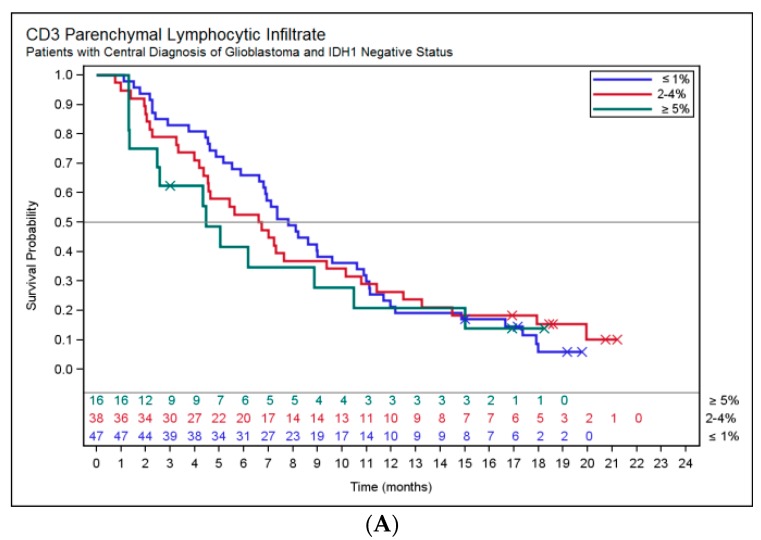
Galunisertib, a Transforming growth factor-βRI (TGF-βRI) kinase inhibitor, blocks TGF-β-mediated tumor growth in glioblastoma. In a three-arm study of galunisertib (300 mg/day) monotherapy (intermittent dosing; each cycle =14 days on/14 days off), lomustine monotherapy, and galunisertib plus lomustine therapy, baseline tumor tissue was evaluated to identify markers associated with tumor stage (e.g., histopathology, Ki67, glial fibrillary acidic protein) and TGF-β-related signaling (e.g., pSMAD2). Other pharmacodynamic assessments included chemokine, cytokine, and T cell subsets alterations. 158 patients were randomized to galunisertib plus lomustine ( = 79), galunisertib ( = 39) and placebo+lomustine ( = 40). In 127 of these patients, tissue was adequate for central pathology review and biomarker work. Isocitrate dehydrogenase () negative glioblastoma patients with baseline pSMAD2⁺ in cytoplasm had median overall survival (OS) 9.5 months vs. 6.9 months for patients with no tumor pSMAD2 expression ( = 0.4574). Eight patients were IDH1 R132H⁺ and had a median OS of 10.4 months compared to 6.9 months for patients with negative IDH1 R132H ( = 0.5452). IDH1 status was associated with numerically higher plasma macrophage-derived chemokine (MDC/CCL22), higher whole blood FOXP3, and reduced tumor CD3⁺ T cell counts. Compared to the baseline, treatment with galunisertib monotherapy preserved CD4⁺ T cell counts, eosinophils, lymphocytes, and the CD4/CD8 ratio. The T-regulatory cell compartment was associated with better OS with MDC/CCL22 as a prominent prognostic marker.
加鲁尼塞替布是一种转化生长因子-βRI(TGF-βRI)激酶抑制剂,可阻断胶质母细胞瘤中TGF-β介导的肿瘤生长。在一项关于加鲁尼塞替布(300毫克/天)单药治疗(间歇给药;每个周期为14天用药/14天停药)、洛莫司汀单药治疗以及加鲁尼塞替布联合洛莫司汀治疗的三臂研究中,对基线肿瘤组织进行了评估,以确定与肿瘤分期相关的标志物(如组织病理学、Ki67、胶质纤维酸性蛋白)和TGF-β相关信号(如pSMAD2)。其他药效学评估包括趋化因子、细胞因子和T细胞亚群的改变。158例患者被随机分为加鲁尼塞替布联合洛莫司汀组(n = 79)、加鲁尼塞替布组(n = 39)和安慰剂+洛莫司汀组(n = 40)。在这些患者中的127例中,组织足以进行中心病理学检查和生物标志物研究。细胞质中基线pSMAD2⁺的异柠檬酸脱氢酶(IDH)阴性胶质母细胞瘤患者的中位总生存期(OS)为9.5个月,而无肿瘤pSMAD2表达的患者为6.9个月(P = 0.4574)。8例患者为IDH1 R132H⁺,中位OS为10.4个月,而IDH1 R132H阴性患者为6.9个月(P = 0.5452)。IDH1状态在数值上与血浆巨噬细胞衍生趋化因子(MDC/CCL22)升高、全血FOXP3升高以及肿瘤CD3⁺T细胞计数减少相关。与基线相比,加鲁尼塞替布单药治疗可维持CD4⁺T细胞计数、嗜酸性粒细胞、淋巴细胞以及CD4/CD8比值。T调节细胞区室与更好的OS相关,MDC/CCL22是一个突出的预后标志物。