McIntosh Amanda M, Tong Suhong, Deakyne Sara J, Davidson Jesse A, Scott Halden F
1Department of Pediatrics, University of Colorado/Children's Hospital Colorado, Aurora, CO. 2Department of Biostatistics, University of Colorado/Children's Hospital Colorado, Aurora, CO. 3Research Informatics, Children's Hospital Colorado, Aurora, CO. 4Department of Pediatrics, Pediatric Cardiology, University of Colorado/Children's Hospital Colorado, Aurora, CO. 5Department of Pediatrics, Pediatric Emergency Medicine, University of Colorado/Children's Hospital Colorado, Aurora, CO.
Pediatr Crit Care Med. 2017 Aug;18(8):750-757. doi: 10.1097/PCC.0000000000001191.
To assess the validity of Vasoactive-Inotropic Score as a scoring system for cardiovascular support and surrogate outcome in pediatric sepsis.
Secondary retrospective analysis of a single-center sepsis registry.
Freestanding children's hospital and tertiary referral center.
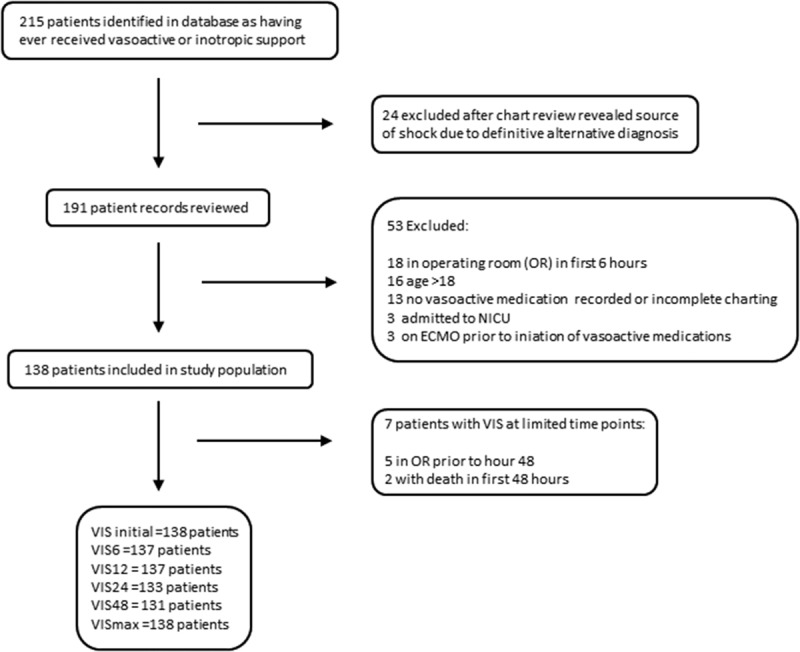
Children greater than 60 days and less than 18 years with sepsis identified in the emergency department between January 2012 and June 2015 treated with at least one vasoactive medication within 48 hours of admission to the PICU.
None.
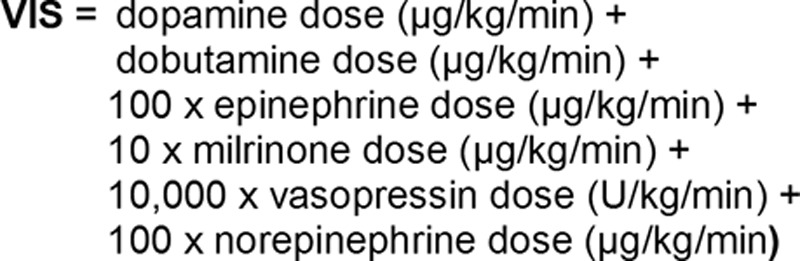
Vasoactive-Inotropic Score was abstracted at 6, 12, 24, and 48 hours post ICU admission. Primary outcomes were ventilator days and ICU length of stay. The secondary outcome was a composite outcome of cardiac arrest/extracorporeal membrane oxygenation/in-hospital mortality. One hundred thirty-eight patients met inclusion criteria. Most common infectious sources were pneumonia (32%) and bacteremia (23%). Thirty-three percent were intubated and mortality was 6%. Of the time points assessed, Vasoactive-Inotropic Score at 48 hours showed the strongest correlation with ICU length of stay (r = 0.53; p < 0.0001) and ventilator days (r = 0.52; p < 0.0001). On multivariable analysis, Vasoactive-Inotropic Score at 48 hours was a strong independent predictor of primary outcomes and intubation. For every unit increase in Vasoactive-Inotropic Score at 48 hours, there was a 13% increase in ICU length of stay (p < 0.001) and 8% increase in ventilator days (p < 0.01). For every unit increase in Vasoactive-Inotropic Score at 12 hours, there was a 14% increase in odds of having the composite outcome (p < 0.01).
Vasoactive-Inotropic Score in pediatric sepsis patients is independently associated with important clinically relevant outcomes including ICU length of stay, ventilator days, and cardiac arrest/extracorporeal membrane oxygenation/mortality. Vasoactive-Inotropic Score may be a useful surrogate outcome in pediatric sepsis.
评估血管活性-正性肌力评分作为小儿脓毒症心血管支持评分系统及替代结局指标的有效性。
对单中心脓毒症登记处进行二次回顾性分析。
独立儿童医院及三级转诊中心。
2012年1月至2015年6月期间在急诊科确诊为脓毒症、年龄大于60天且小于18岁、入住儿科重症监护病房(PICU)48小时内至少接受过一种血管活性药物治疗的儿童。
无。
在入住ICU后6、12、24和48小时提取血管活性-正性肌力评分。主要结局指标为机械通气天数和ICU住院时间。次要结局指标为心脏骤停/体外膜肺氧合/院内死亡的复合结局。138例患者符合纳入标准。最常见的感染源为肺炎(32%)和菌血症(23%)。33%的患者接受了气管插管,死亡率为6%。在评估的时间点中,48小时时的血管活性-正性肌力评分与ICU住院时间(r = 0.53;p < 0.0001)和机械通气天数(r = 0.52;p < 0.0001)的相关性最强。多变量分析显示,48小时时的血管活性-正性肌力评分是主要结局指标和气管插管的强有力独立预测因素。48小时时血管活性-正性肌力评分每增加一个单位,ICU住院时间增加13%(p < 0.001),机械通气天数增加8%(p < 0.01)。12小时时血管活性-正性肌力评分每增加一个单位,出现复合结局的几率增加14%(p < 0.01)。
小儿脓毒症患者的血管活性-正性肌力评分与包括ICU住院时间、机械通气天数以及心脏骤停/体外膜肺氧合/死亡率等重要的临床相关结局独立相关。血管活性-正性肌力评分可能是小儿脓毒症中一个有用的替代结局指标。