Balsells Evelyn, Guillot Laurence, Nair Harish, Kyaw Moe H
Usher Institute of Population Health Sciences and Informatics, University of Edinburgh, Medical School, Teviot Place, Edinburgh, United Kingdom.
Sanofi Pasteur, Swiftwater, Pennsylvania, United States of America.
PLoS One. 2017 May 9;12(5):e0177113. doi: 10.1371/journal.pone.0177113. eCollection 2017.
Routine immunisation with pneumococcal conjugate vaccines (PCV7/10/13) has reduced invasive pneumococcal disease (IPD) due to vaccine serotypes significantly. However, an increase in disease due to non-vaccine types, or serotype replacement, has been observed. Serotypes' individual contributions to IPD play a critical role in determining the overall effects of PCVs. This study examines the distribution of pneumococcal serotypes in children to identify leading serotypes associated with IPD post-PCV introduction.
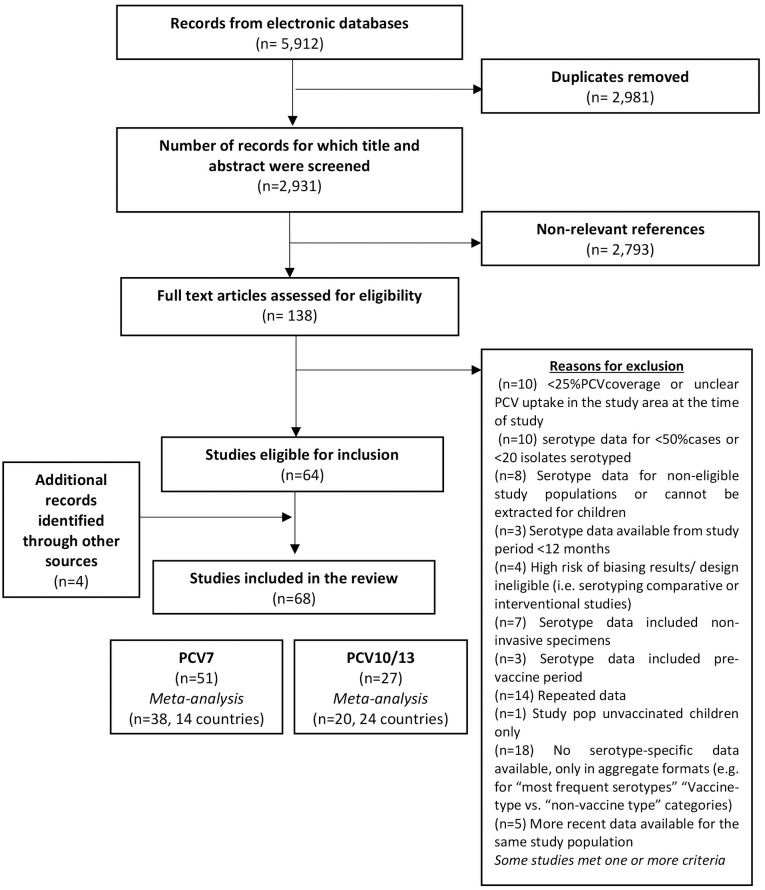
A systematic search was performed to identify studies and surveillance reports (published between 2000 and December 2015) of pneumococcal serotypes causing childhood IPD post-PCV introduction. Serotype data were differentiated based on the PCV administered during the study period: PCV7 or higher valent PCVs (PCV10 or PCV13). Meta-analysis was conducted to estimate the proportional contributions of the most frequent serotypes in childhood IPD in each period.
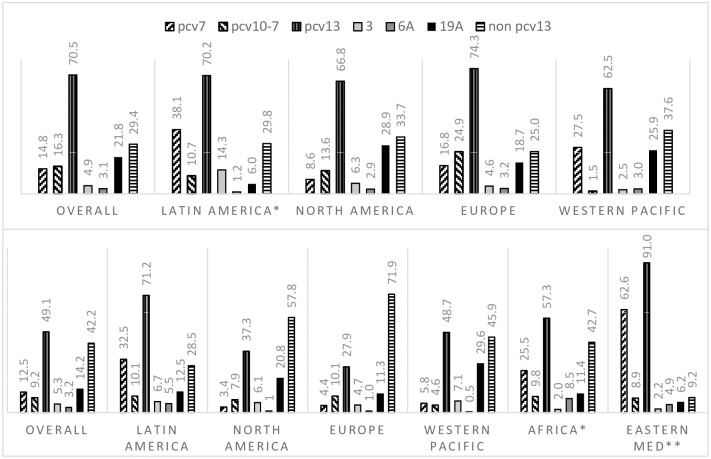
We identified 68 studies reporting serotype data among IPD cases in children. We analysed data from 38 studies (14 countries) where PCV7 was administered and 20 (24 countries) where PCV10 or PCV13 have been introduced. Studies reported early and late periods of PCV7 administration (range: 2001∓13). In these settings, serotype 19A was the most predominant cause of childhood IPD, accounting for 21.8% (95%CI 18.6∓25.6) of cases. In countries that have introduced higher valent PCVs, study periods were largely representative of the transition and early years of PCV10 or PCV13. In these studies, the overall serotype-specific contribution of 19A was lower (14.2% 95%CI 11.1∓18.3). Overall, non-PCV13 serotypes contributed to 42.2% (95%CI 36.1∓49.5%) of childhood IPD cases. However, regional differences were noted (57.8% in North America, 71.9% in Europe, 45.9% in Western Pacific, 28.5% in Latin America, 42.7% in one African country, and 9.2% in one Eastern Mediterranean country). Predominant non-PCV13 serotypes overall were 22F, 12F, 33F, 24F, 15C, 15B, 23B, 10A, and 38 (descending order), but their rank order varied by region.
Childhood IPD is associated with a wide number of serotypes. In the early years after introduction of higher valent PCVs, non-PCV13 types caused a considerable proportion of childhood IPD. Serotype data, particularly from resource-limited countries with high burden of IPD, are needed to assess the importance of serotypes in different settings. The geographic diversity of pneumococcal serotypes highlights the importance of continued surveillance to guide vaccine design and recommendations.
使用肺炎球菌结合疫苗(PCV7/10/13)进行常规免疫接种已显著降低了由疫苗血清型引起的侵袭性肺炎球菌疾病(IPD)。然而,已观察到非疫苗血清型引起的疾病增加,即血清型替换现象。血清型对IPD的个体贡献在确定肺炎球菌结合疫苗(PCV)的总体效果方面起着关键作用。本研究调查了儿童肺炎球菌血清型的分布情况,以确定在引入PCV后与IPD相关的主要血清型。
进行了系统检索,以识别有关在引入PCV后导致儿童IPD的肺炎球菌血清型的研究和监测报告(发表于2000年至2015年12月之间)。血清型数据根据研究期间所接种的PCV进行区分:PCV7或更高价的PCV(PCV10或PCV13)。进行荟萃分析以估计每个时期儿童IPD中最常见血清型的比例贡献。
我们识别出68项报告儿童IPD病例血清型数据的研究。我们分析了来自38项研究(14个国家)的数据,这些研究中使用了PCV7,以及20项研究(24个国家)的数据,这些研究中引入了PCV10或PCV13。研究报告了PCV7接种的早期和后期(范围:2001年至2013年)。在这些情况下,19A血清型是儿童IPD的最主要病因,占病例的21.8%(95%置信区间18.6%至25.6%)。在引入更高价PCV的国家中,研究时期在很大程度上代表了PCV10或PCV13的过渡阶段及早期。在这些研究中,19A血清型的总体血清型特异性贡献较低(14.2%,95%置信区间11.1%至18.3%)。总体而言,非PCV13血清型占儿童IPD病例的42.2%(95%置信区间36.1%至49.5%)。然而,存在地区差异(北美为57.8%,欧洲为71.9%,西太平洋为45.9%t,拉丁美洲为28.5%,一个非洲国家为42.7%,一个东地中海国家为9.2%)。总体而言,主要的非PCV13血清型依次为22F、12F、33F、24F、15C、15B、23B、10A和38,但它们的排名顺序因地区而异。
儿童IPD与多种血清型相关。在引入更高价PCV后的早期,非PCV13血清型导致了相当比例的儿童IPD。需要血清型数据,特别是来自IPD负担高的资源有限国家的数据,以评估血清型在不同环境中的重要性。肺炎球菌血清型的地理多样性凸显了持续监测以指导疫苗设计和建议的重要性。