Moore Kerryn A, Fowkes Freya J I, Wiladphaingern Jacher, Wai Nan San, Paw Moo Kho, Pimanpanarak Mupawjay, Carrara Verena I, Raksuansak Jathee, Simpson Julie A, White Nicholas J, Nosten François, McGready Rose
Centre for Epidemiology and Biostatistics, Melbourne School of Population and Global Health, The University of Melbourne, Melbourne, VIC, Australia.
Macfarlane Burnet Institute for Medical Research and Public Health, Melbourne, VIC, Australia.
BMC Med. 2017 May 10;15(1):98. doi: 10.1186/s12916-017-0863-z.
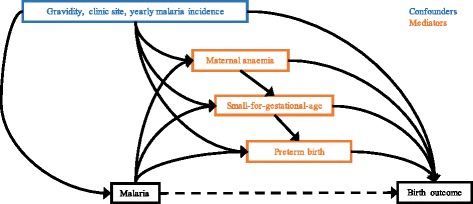
Malaria in pregnancy is preventable and contributes significantly to the estimated 5.5 million stillbirths and neonatal deaths that occur annually. The contribution of malaria in pregnancy in areas of low transmission has not been quantified, and the roles of maternal anaemia, small-for-gestational-age status, and preterm birth in mediating the effect of malaria in pregnancy on stillbirth and neonatal death are poorly elucidated.
We analysed observational data routinely collected at antenatal clinics on the Thai-Myanmar border (1986-2015). We used Cox regression and sequential mediation analysis to determine the effect of falciparum and vivax malaria in pregnancy on antepartum (death in utero) and intrapartum (death during labour) stillbirth and neonatal mortality as well as mediation through maternal anaemia, preterm birth, and small-for-gestational-age status.
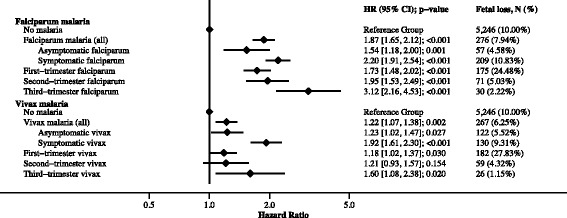
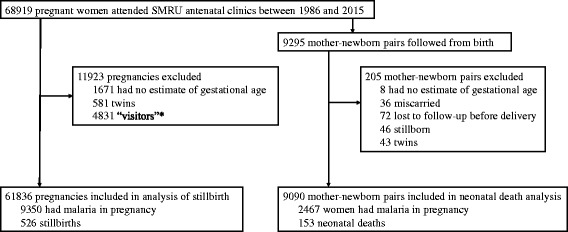
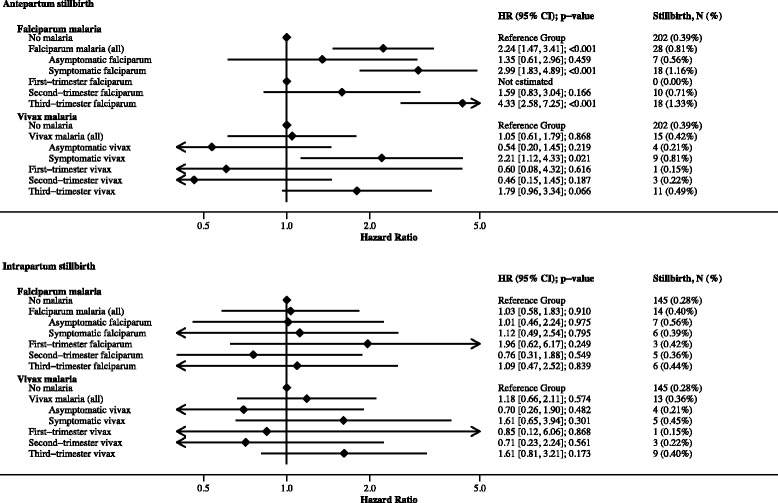
Of 61,836 women, 9350 (15%) had malaria in pregnancy, and 526 (0.8%) had stillbirths. In a sub-set of 9090 live born singletons followed from birth there were 153 (1.7%) neonatal deaths. The hazard of antepartum stillbirth increased 2.24-fold [95% confidence interval: 1.47, 3.41] following falciparum malaria (42% mediated through small-for-gestational-age status and anaemia), driven by symptomatic falciparum malaria (hazard ratio, HR: 2.99 [1.83, 4.89]) rather than asymptomatic falciparum malaria (HR: 1.35 [0.61, 2.96]). The hazard of antepartum stillbirth increased 2.21-fold [1.12, 4.33] following symptomatic vivax malaria (24% mediated through small-for-gestational-age status and anaemia) but not asymptomatic vivax malaria (HR: 0.54 [0.20, 1.45]). There was no association between falciparum or vivax malaria in pregnancy and intrapartum stillbirth (falciparum HR: 1.03 [0.58, 1.83]; vivax HR: 1.18 [0.66, 2.11]). Falciparum and vivax malaria in pregnancy increased the hazard of neonatal death 2.55-fold [1.54, 4.22] and 1.98-fold [1.10, 3.57], respectively (40% and 50%, respectively, mediated through small-for-gestational-age status and preterm birth).
Prevention of malaria in pregnancy, new and existing interventions to prevent small-for-gestational-age status and maternal anaemia, and improved capacity for managing preterm and small-for-gestational-age newborns will reduce the number of malaria-associated stillbirths and neonatal deaths in malaria-endemic areas.
妊娠疟疾是可预防的,每年约550万死产和新生儿死亡中,妊娠疟疾起了很大作用。低传播地区妊娠疟疾的影响尚未量化,妊娠疟疾通过母体贫血、小于胎龄状态和早产导致死产和新生儿死亡的作用也未得到充分阐明。
我们分析了泰国-缅甸边境产前诊所常规收集的观察性数据(1986 - 2015年)。我们使用Cox回归和序贯中介分析来确定妊娠期间恶性疟和间日疟对产前(子宫内死亡)和产时(分娩期间死亡)死产及新生儿死亡率的影响,以及通过母体贫血、早产和小于胎龄状态的中介作用。
在61836名妇女中,9350名(15%)妊娠期间患疟疾,526名(0.8%)发生死产。在9090名单胎活产儿出生后随访的子集中,有153名(1.7%)新生儿死亡。恶性疟后产前死产风险增加2.24倍[95%置信区间:1.47, 3.41](42%通过小于胎龄状态和贫血介导),由有症状的恶性疟驱动(风险比,HR:2.99 [1.83, 4.89]),而非无症状恶性疟(HR:1.35 [0.61, 2.96])。有症状的间日疟后产前死产风险增加2.21倍[1.12, 4.33](24%通过小于胎龄状态和贫血介导),但无症状间日疟无此关联(HR:0.54 [0.20, 1.45])。妊娠期间恶性疟或间日疟与产时死产无关联(恶性疟HR:1.03 [0.58, 1.83];间日疟HR:1.18 [0.66, 2.11])。妊娠期间恶性疟和间日疟分别使新生儿死亡风险增加2.55倍[1.54, 4.22]和1.98倍[1.10, 3.57](分别有40%和50%通过小于胎龄状态和早产介导)。
预防妊娠疟疾、预防小于胎龄状态和母体贫血的新老干预措施,以及提高管理早产和小于胎龄新生儿的能力,将减少疟疾流行地区与疟疾相关的死产和新生儿死亡数量。