Department of Internal Medicine, Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan.
Division of Pulmonary and Critical Care Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan.
BMC Pharmacol Toxicol. 2017 May 10;18(1):21. doi: 10.1186/s40360-017-0130-0.
Epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs) such as gefitinib can provide better efficacy and prolonged progression free survival (PFS) than cytotoxic chemotherapy for metastatic lung non-squamous cell carcinoma harboring susceptible EGFR mutations when used as first-line therapy. Cytotoxic chemotherapy is regarded as being the standard therapy to overcome acquired resistance to an initial EGFR TKI. However, there is currently no consensus on how best to treat patients who develop resistance to both an initial EGFR TKI and chemotherapy.
We enrolled stage IV lung adenocarcinoma patients with an EGFR mutation and who had developed acquired resistance to gefitinib and cytotoxic chemotherapy from two university-affiliated hospitals in Taiwan from June 2011 to December 2014. Basic demographic data, included Eastern Cooperative Oncology Group (ECOG) performance status were collected, and the response rate, progression-free survival (PFS) and overall survival (OS) were analyzed.
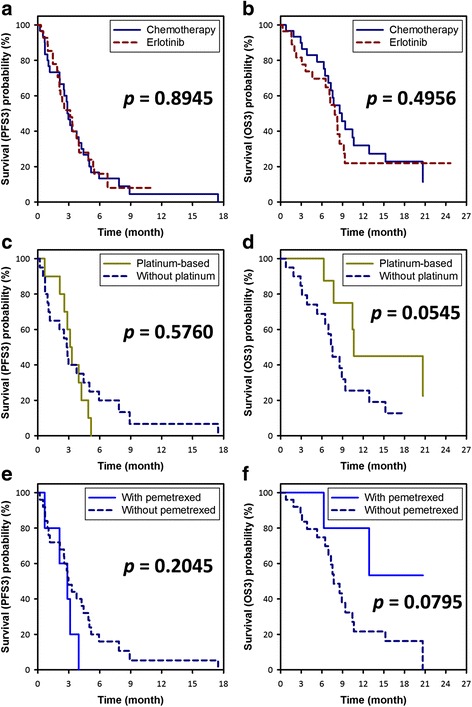
Two hundred and nine patients with mutated EGFR and who took gefitinib as the first-line therapy were identified in the study period, of whom 86 received second-line cytotoxic chemotherapy, and 60 who received third-line therapy were eligible for this study. The patients who received cytotoxic chemotherapy had a significantly higher disease control rate than those who received erlotinib (73% vs. 46%, p = 0.0363), however there were no significant differences in PFS (2.9 months vs. 3.1 months, p = 0.9049) and OS (8.9 months vs. 7.9 months, p = 0.4956). Platinum- or pemetrexed-based chemotherapy provided similar PFS and OS as others did. The only significant poor prognostic factors for OS were old age (≥65 years) (HR = 5.97 [2.65-13.44], p < 0.0001) and poor performance status (ECOG ≥2) (HR = 5.84 [2.61-13.09], p < 0.0001).
Retreatment with an EGFR TKI is not inferior to cytotoxic chemotherapy when used as salvage therapy for patients with adenocarcinoma with an EGFR mutation, especially if a third-generation EGFR TKI is not available, or if the reason for resistance is unknown or is not related to the T790M mutation. Old age and poor ECOG score were both poor prognostic factors in the salvage therapy.
表皮生长因子受体酪氨酸激酶抑制剂(EGFR-TKIs),如吉非替尼,在转移性肺非鳞状细胞癌中,与敏感的 EGFR 突变相比,可提供更好的疗效和延长无进展生存期(PFS),可作为一线治疗。细胞毒性化疗被认为是克服初始 EGFR TKI 获得性耐药的标准治疗方法。然而,目前对于如何最好地治疗初始 EGFR TKI 和化疗均耐药的患者尚无共识。
我们招募了来自台湾两家大学附属医院的 2011 年 6 月至 2014 年 12 月期间患有 EGFR 突变且对吉非替尼和细胞毒性化疗产生获得性耐药的 IV 期肺腺癌患者。收集了基本的人口统计学数据,包括东部合作肿瘤学组(ECOG)表现状态,并分析了缓解率、无进展生存期(PFS)和总生存期(OS)。
在研究期间,确定了 209 例接受 EGFR 突变的吉非替尼一线治疗的患者,其中 86 例接受二线细胞毒性化疗,60 例接受三线治疗的患者符合本研究标准。接受细胞毒性化疗的患者疾病控制率显著高于接受厄洛替尼的患者(73%比 46%,p=0.0363),但 PFS(2.9 个月比 3.1 个月,p=0.9049)和 OS(8.9 个月比 7.9 个月,p=0.4956)无显著差异。基于铂类或培美曲塞的化疗提供了与其他化疗相似的 PFS 和 OS。OS 的唯一显著不良预后因素是年龄较大(≥65 岁)(HR=5.97[2.65-13.44],p<0.0001)和 ECOG 状态较差(≥2)(HR=5.84[2.61-13.09],p<0.0001)。
对于 EGFR 突变的腺癌患者,EGFR TKI 作为挽救性治疗的疗效并不逊于细胞毒性化疗,特别是如果没有第三代 EGFR TKI,或者耐药的原因不明或与 T790M 突变无关。年龄较大和 ECOG 评分较差均是挽救性治疗的不良预后因素。