Habib Shahid, Khan Khalid, Hsu Chiu-Hsieh, Meister Edward, Rana Abbas, Boyer Thomas
Liver Institute, PLLC, 2830 North Swan Road, Suite 180, Tucson, AZ 85712, USA.
Transplant Institute, MedStar Georgetown University Hospital, 3800 Reservoir Rd, Main, Washington, DC 20007, USA.
Gastroenterology Res. 2017 Apr;10(2):106-115. doi: 10.14740/gr803w. Epub 2017 Apr 19.
We evaluated the concept of whether liver failure patients with a superimposed kidney injury receiving a simultaneous liver and kidney transplant (SLKT) have similar outcomes compared to patients with liver failure without a kidney injury receiving a liver transplantation (LT) alone.
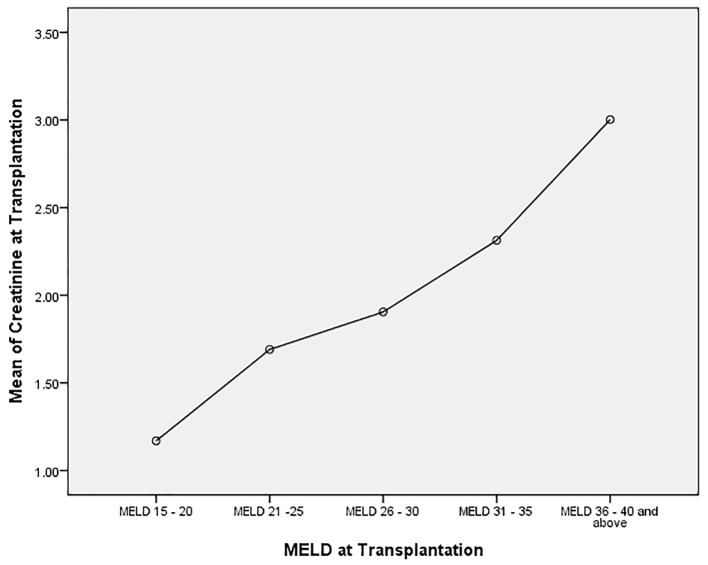
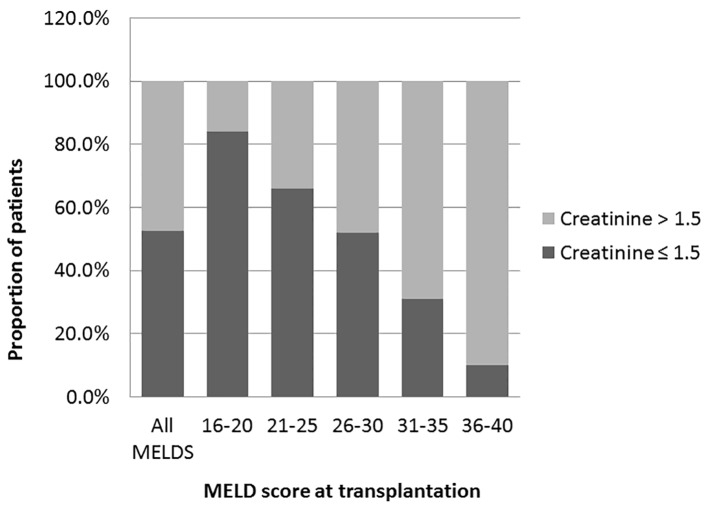
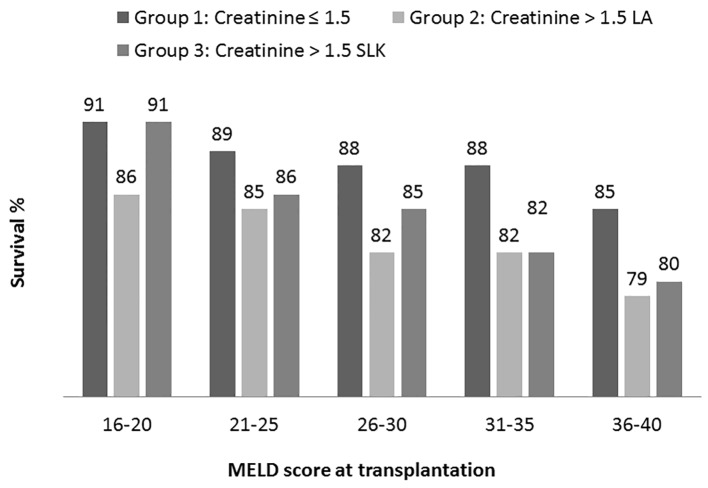
Using data from the United Network of Organ Sharing (UNOS) database, patients were divided into five groups based on pre-transplant model for end-stage liver disease (MELD) scores and categorized as not having (serum creatinine (sCr) ≤ 1.5 mg/dL) or having (sCr > 1.5 mg/dL) renal dysfunction. Of 30,958 patients undergoing LT, 14,679 (47.5%) had renal dysfunction, and of those, 5,084 (16.4%) had dialysis.
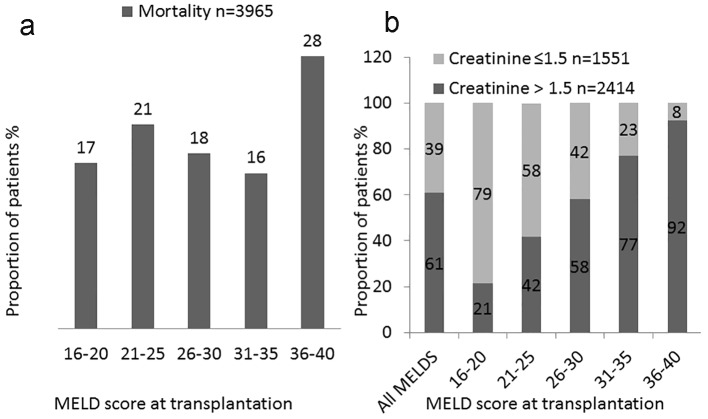
Survival in those (liver failure with renal dysfunction) receiving SLKT was significantly worse (P < 0.001) as compared to those with sCr < 1.5 mg/dL (liver failure only). The highest mortality rate observed was 21% in the 36+ MELD group with renal dysfunction with or without SLKT. In high MELD recipients (MELD > 30) with renal dysfunction, presence of renal dysfunction affects the outcome and SLKT does not improve survival. In low MELD recipients (16 - 20), presence of renal dysfunction at the time of transplantation does affect post-transplant survival, but survival is improved with SLKT.
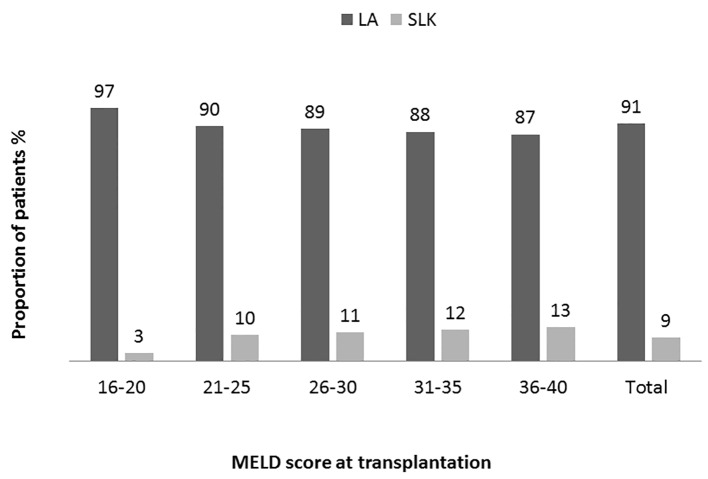
SLKT improved 1-year survival only in low MELD (16 - 20) recipients but not in other groups. Performance of SLKT should be limited to patients where a benefit in survival and post-transplant outcomes can be demonstrated.
我们评估了一个概念,即与单纯接受肝移植(LT)的无肾损伤肝衰竭患者相比,同时接受肝肾移植(SLKT)的合并肾损伤的肝衰竭患者是否具有相似的预后。
利用器官共享联合网络(UNOS)数据库的数据,根据移植前终末期肝病模型(MELD)评分将患者分为五组,并根据是否存在肾功能不全(血清肌酐(sCr)≤1.5mg/dL)或存在肾功能不全(sCr>1.5mg/dL)进行分类。在30958例接受肝移植的患者中,14679例(47.5%)存在肾功能不全,其中5084例(16.4%)接受透析治疗。
与sCr<1.5mg/dL(仅肝衰竭)的患者相比,接受SLKT的患者(肝衰竭合并肾功能不全)的生存率显著更差(P<0.001)。观察到的最高死亡率为36+MELD组中存在或不存在肾功能不全且接受SLKT的患者中的21%。在合并肾功能不全的高MELD受者(MELD>30)中,肾功能不全的存在影响预后,SLKT并不能提高生存率。在低MELD受者(16-20)中,移植时肾功能不全的存在确实会影响移植后的生存率,但SLKT可提高生存率。
SLKT仅改善了低MELD(16-20)受者的1年生存率,而其他组未改善。SLKT的应用应仅限于能够证明对生存率和移植后预后有益的患者。