De Brauwer Isabelle, Cornette Pascale, Boland Benoît, Verschuren Franck, D'Hoore William
Institute of Health and Society (IRSS), Université catholique de Louvain, Brussels, Belgium.
Department of Geriatric Medicine, Cliniques universitaires Saint Luc, Brussels, Belgium.
BMC Geriatr. 2017 May 12;17(1):105. doi: 10.1186/s12877-017-0498-0.
In the Emergency Department (ED), early and rapid identification of older people at risk of adverse outcomes, who could best benefit from complex geriatric intervention, would avoid wasting time, especially in terms of prevention of adverse outcomes, and ensure optimal orientation of vulnerable patients. We wanted to test the predictive ability of a screening tool assessing risk of functional decline (FD), named SHERPA, 10 years after its conception, and to assess the added value of other clinical or biological factors associated with FD.
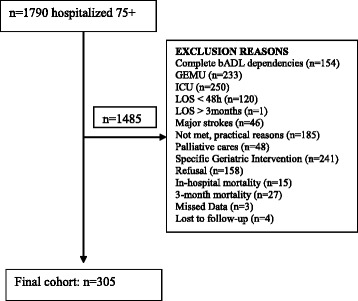
A prospective cohort study of older patients (n = 305, ≥ 75 years) admitted through the emergency department, for at least 48 h in non-geriatric wards (mean age 82.5 ± 4.9, 55% women). SHERPA variables (i.e. age, pre-admission instrumental Activity of Daily Living (ADL) status, falls within a year, self-rated health and 21-point MMSE) were collected within 48 h of admission, along with socio-demographic, medical and biological data. Functional status was followed at 3 months by phone. FD was defined as a decrease at 3 months of at least one point in the pre-admission basic ADL score. Predictive ability of SHERPA was assessed using c-statistic, predictive values and likelihood ratios. Measures of discrimination improvement were Net Reclassification Improvement and Integrated Discrimination Improvement.
One hundred and five patients (34%) developed 3-month FD. Predictive ability of SHERPA decreased dramatically over 10 years (c = 0.73 vs. 0.64). Only two of its constitutive variables, i.e. falls and instrumental ADL, were significant in logistic regression analysis for functional decline, while 21-point MMSE was kept in the model for clinical relevance. Demographic, comorbidity or laboratory data available upon admission did not improve the SHERPA predictive yield.
Prediction of FD with SHERPA is difficult, but predictive factors, i.e. falls, pre-existing functional limitation and cognitive impairment, stay consistent across time and with literature. As accuracy of SHERPA and others existing screening tools for FD is moderate, using these predictors as flags instead of using composite scales can be a way to screen for high-risk patients.
在急诊科,尽早且快速地识别出可能从复杂老年病干预中获益最大的有不良结局风险的老年人,可避免时间浪费,尤其是在预防不良结局方面,并确保对脆弱患者进行最佳引导。我们想要在名为SHERPA的评估功能衰退(FD)风险的筛查工具问世10年后,测试其预测能力,并评估与FD相关的其他临床或生物学因素的附加价值。
一项对通过急诊科收治的老年患者(n = 305,≥75岁)进行的前瞻性队列研究,这些患者在非老年病房至少住院48小时(平均年龄82.5±4.9岁,55%为女性)。在入院48小时内收集SHERPA变量(即年龄、入院前工具性日常生活活动(ADL)状态、一年内跌倒情况、自评健康状况和21分简易精神状态检查表(MMSE)),以及社会人口统计学、医学和生物学数据。在3个月时通过电话随访功能状态。FD被定义为入院前基本ADL评分在3个月时至少下降1分。使用c统计量、预测值和似然比评估SHERPA的预测能力。判别改善的指标是净重新分类改善和综合判别改善。
105名患者(34%)出现了3个月时的FD。SHERPA的预测能力在10年中显著下降(c = 0.73对0.64)。在功能衰退的逻辑回归分析中,其构成变量中只有两个,即跌倒和工具性ADL,具有显著意义,而21分MMSE因临床相关性被保留在模型中。入院时可用的人口统计学、合并症或实验室数据并未提高SHERPA的预测效能。
用SHERPA预测FD很困难,但预测因素,即跌倒、既往功能受限和认知障碍,在不同时间以及与文献相比保持一致。由于SHERPA和其他现有的FD筛查工具的准确性中等,将这些预测因素用作警示标志而非使用综合量表可能是筛查高危患者的一种方法。