Huang Gui-Qian, Zheng Ji-Na, Zou Tian-Tian, Chen Yi-Ran, Shi Ke-Qing, Poucke Sven Van, Cheng Zhang, Ruan Lu-Yi, Zheng Ming-Hua
Department of Hepatology, Liver Research Center, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China.
Renji School of Wenzhou Medical University, Wenzhou, China.
J Clin Transl Hepatol. 2017 Mar 28;5(1):35-42. doi: 10.14218/JCTH.2016.00035. Epub 2017 Feb 25.
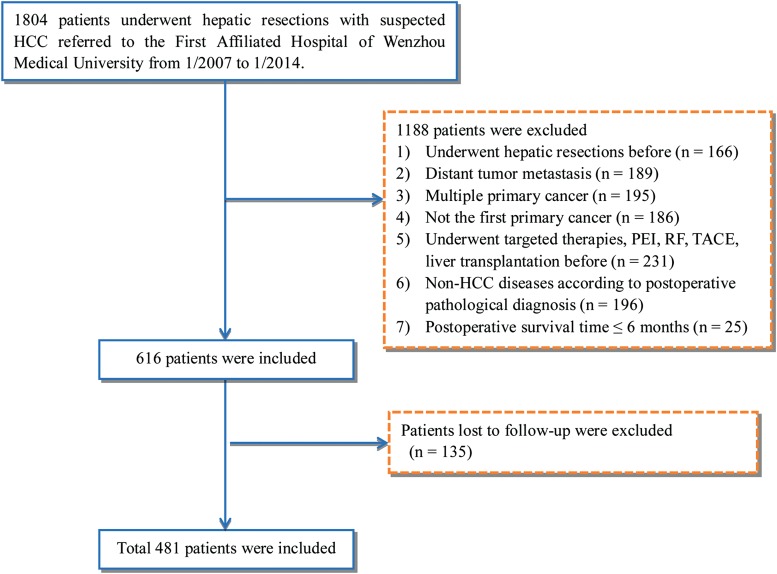
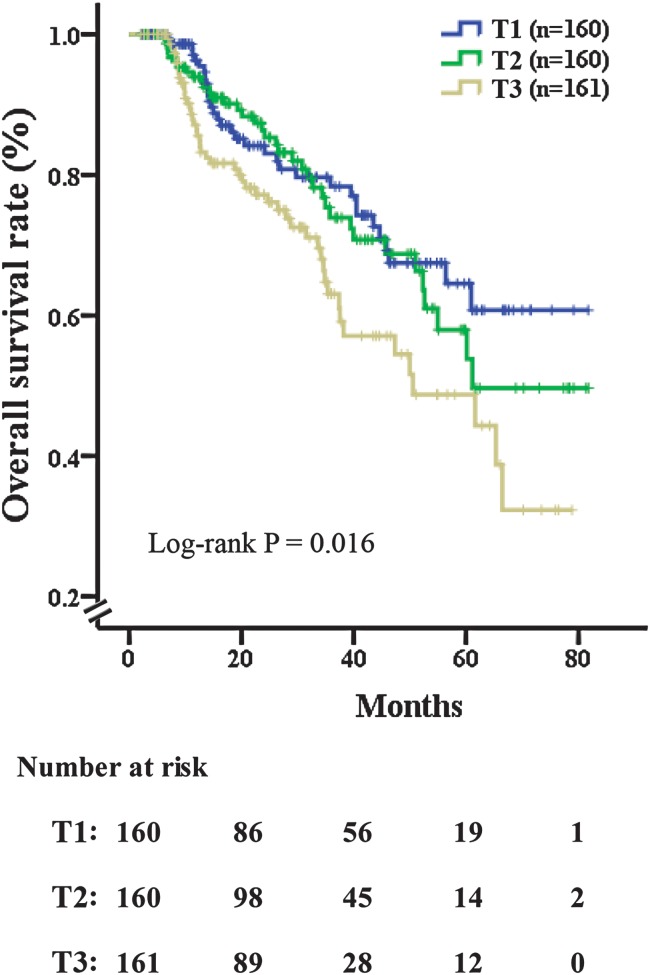
Platelet-to-lymphocyte ratio (PLR) has been shown to predict prognosis of cancers. We aimed to evaluate the prognostic value of stratification of PLR in patients after curative liver resection (CLR) for hepatocellular carcinoma (HCC). A total of 1804 patients who underwent CLR for suspected HCC between January 2007 and January 2014 were screened for the study. All of the patients were categorized into equal tertiles according to the number of patients and the distribution of PLR. Prognostic significance was determined for overall survival (OS) and was assessed using Kaplan-Meier analysis. Univariate and multivariate Cox proportional hazard regression analyses were evaluated for association of all independent parameters with disease prognosis. The optimal cut-off points of preoperative PLR were: (T1) 11.98-75.00, (T2) 75.00-113.33 and (T3) 113.33-567.50. There were obvious differences in each PLR tertile with mortality within 36 months of CLR ( < 0.001). Multivariable analysis suggested that the level of PLR (HR = 1.004, 95%CI: 1.001-1.008, = 0.006), portal vein thrombosis (HR = 3.406, 95%CI: 1.185-9.794, = 0.023), number of nodules (HR = 1.810, 95%CI: 1.345-2.437, < 0.001), Child-Turcotte-Pugh score (HR = 1.741, 95%CI: 1.129-2.684, = 0.012) and microvascular invasion (HR = 2.730, 95%CI: 1.777-4.196, < 0.001) were significant predictors of mortality. Kaplan-Meier analysis of overall survival (OS) demonstrated that each PLR tertile showed a progressively worse OS and apparent separation ( = 0.016). The highest 5-year OS rate following CLR (58%) was revealed in tertile 1. In contrast, the lowest 5-year OS rate (30%) was revealed in tertile 3. Stratified preoperative PLR could strengthen the predictive power for OS in HCC patients with CLR.
血小板与淋巴细胞比值(PLR)已被证明可预测癌症预后。我们旨在评估肝细胞癌(HCC)根治性肝切除(CLR)术后患者PLR分层的预后价值。对2007年1月至2014年1月期间因疑似HCC接受CLR的1804例患者进行了研究筛选。根据患者数量和PLR分布将所有患者分为三等分。确定总生存期(OS)的预后意义,并使用Kaplan-Meier分析进行评估。对所有独立参数与疾病预后的关联进行单因素和多因素Cox比例风险回归分析。术前PLR的最佳截断点为:(T1)11.98 - 75.00,(T2)75.00 - 113.33,(T3)113.33 - 567.50。CLR术后36个月内各PLR三分位数组的死亡率存在明显差异(<0.001)。多变量分析表明,PLR水平(HR = 1.004,95%CI:1.001 - 1.008,P = 0.006)、门静脉血栓形成(HR = 3.406,95%CI:1.185 - 9.794,P = 0.023)、结节数量(HR = 1.810,95%CI:1.345 - 2.437,P < 0.001)、Child-Turcotte-Pugh评分(HR = 1.741,95%CI:1.129 - 2.684,P = 0.012)和微血管侵犯(HR = 2.730,95%CI:1.777 - 4.196,P < 0.001)是死亡率的重要预测因素。总生存期(OS)的Kaplan-Meier分析表明,各PLR三分位数组的OS逐渐变差且有明显分离(P = 0.016)。CLR术后最高的5年总生存率(58%)出现在三分位数1组。相比之下,三分位数3组的5年总生存率最低(30%)。术前PLR分层可增强CLR的HCC患者OS的预测能力。