Gelpi Marco, Hartling Hans J, Ueland Per M, Ullum Henrik, Trøseid Marius, Nielsen Susanne D
Viro-Immunology Research Unit, Department of Infectious Diseases, University Hospital of Copenhagen, Rigshospitalet, Blegdamsvej 9, Copenhagen, Denmark.
Section for pharmacology, Department of Clinical Science, University of Bergen, Bergen, Norway.
BMC Infect Dis. 2017 May 16;17(1):349. doi: 10.1186/s12879-017-2456-z.
Kynurenine/Tryptophan ratio (KTR) is increased in HIV infection, and linked to immune activation. We hypothesized that early cART initiation results in lower KTR compared to late initiation. Furthermore, we hypothesized that KTR prior to cART is a predictor of the magnitude of subsequent reduction in immune activation.
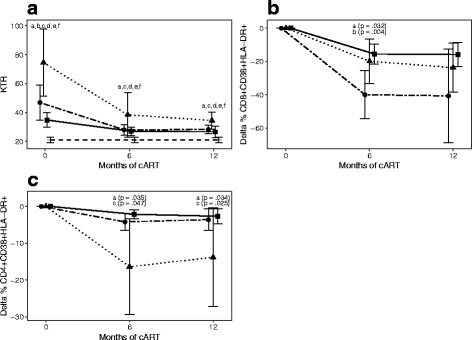
Prospective study including 57 HIV-infected individuals (primary HIV infection (N = 14), early presenters (>350 CD4+ T cells/μL, N = 24), late presenters (<200 CD4+ T cells/μL, N = 19)). Kynurenine and tryptophan were analysed by liquid chromatography-tandem mass spectrometry. Total CD4+ and CD8+ T cells were determined and proportion of activated CD38 + HLA-DR+ Tcells was measured using flow cytometry at baseline and after 6 and 12 months of cART.
At baseline, primary HIV infection had higher KTR than early presenters. However, similar KTR in primary HIV infection and early presenters was found after cART initiation, while late presenters had higher KTR at all time points. In primary HIV infection and early presenters, KTR was positively associated with proportion of activated cells at baseline. Furthermore, in early presenters the KTR at baseline was associated with proportion of activated cells after 6 and 12 months. Interestingly, in primary HIV infection the KTR at baseline was positively associated with reduction in proportion of CD8 + CD38 + HLA-DR T cells after 6 and 12 months.
Lower kynurenine/tryptophan ratio during follow-up was found after early initiation of cART. KTR in primary HIV infection and early presenters was positively associated with immune activation. Importantly, KTR in primary HIV infection predicted the magnitude of subsequent reduction in immune activation. Thus, a beneficial effect of early cART on KTR was suggested.
犬尿氨酸/色氨酸比值(KTR)在HIV感染中升高,并与免疫激活相关。我们假设与延迟启动相比,早期启动抗逆转录病毒治疗(cART)会导致更低的KTR。此外,我们假设cART治疗前的KTR是随后免疫激活降低幅度的一个预测指标。
前瞻性研究纳入了57名HIV感染者(原发性HIV感染(N = 14)、早期就诊者(CD4+ T细胞>350个/μL,N = 24)、晚期就诊者(CD4+ T细胞<200个/μL,N = 19))。采用液相色谱-串联质谱法分析犬尿氨酸和色氨酸。在基线以及cART治疗6个月和12个月后,通过流式细胞术测定总CD4+和CD8+ T细胞,并检测活化的CD38+HLA-DR+ T细胞的比例。
在基线时,原发性HIV感染的KTR高于早期就诊者。然而,在开始cART治疗后,原发性HIV感染和早期就诊者的KTR相似,而晚期就诊者在所有时间点的KTR都更高。在原发性HIV感染和早期就诊者中,基线时KTR与活化细胞比例呈正相关。此外,在早期就诊者中,基线时的KTR与6个月和12个月后的活化细胞比例相关。有趣的是,在原发性HIV感染中,基线时的KTR与6个月和12个月后CD8+CD38+HLA-DR T细胞比例的降低呈正相关。
早期启动cART治疗后,随访期间发现犬尿氨酸/色氨酸比值较低。原发性HIV感染和早期就诊者的KTR与免疫激活呈正相关。重要的是,原发性HIV感染中的KTR预测了随后免疫激活降低的幅度。因此,提示早期cART对KTR有有益作用。