Mullie Guillaume A, Schwartzman Kevin, Zwerling Alice, N'Diaye Dieynaba S
Respiratory Epidemiology and Clinical Research Unit, Montreal Chest Institute, Montreal, QC, Canada.
Faculty of Medicine, McGill University, Montreal, QC, Canada.
BMC Med. 2017 May 17;15(1):104. doi: 10.1186/s12916-017-0865-x.
In North America, tuberculosis incidence is now very low and risk to healthcare workers has fallen. Indeed, recent cohort data question routine annual tuberculosis screening in this context. We compared the cost-effectiveness of three potential strategies for ongoing screening of North American healthcare workers at risk of exposure. The analysis did not evaluate the cost-effectiveness of screening at hiring, and considered only workers with negative baseline tests.
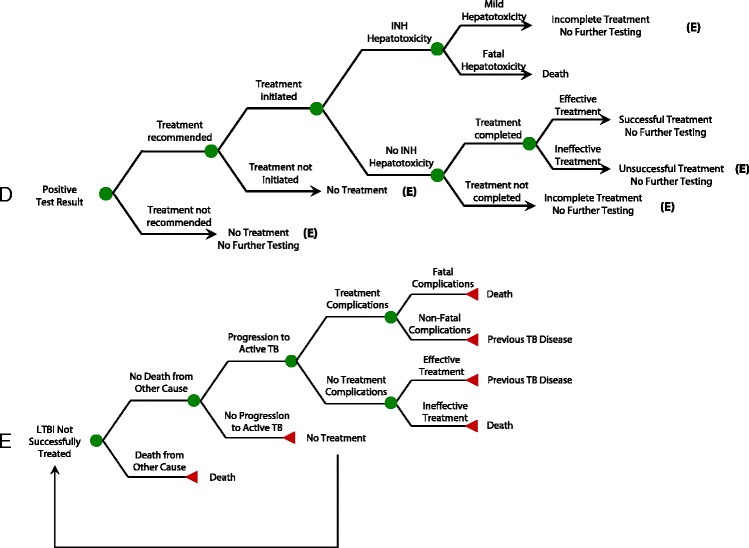
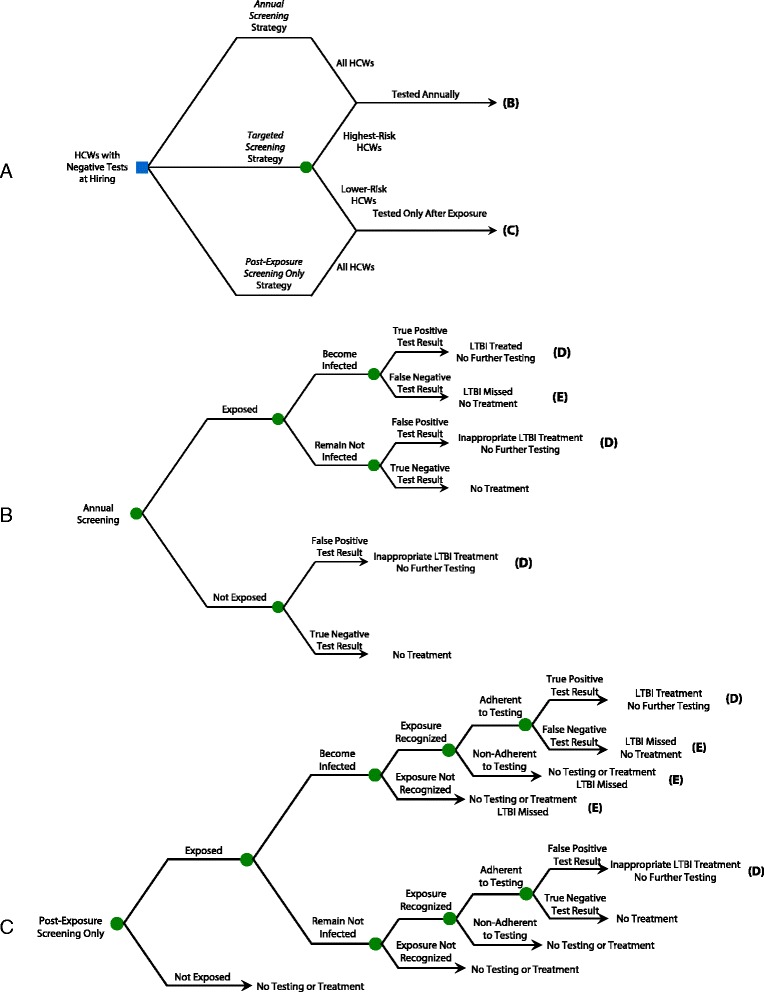
A decision analysis model simulated a hypothetical cohort of 1000 workers following negative baseline tests, considering duties, tuberculosis exposure, testing and treatment. Two tests were modelled, the tuberculin skin test (TST) and QuantiFERON®-TB-Gold In-Tube (QFT). Three screening strategies were compared: (1) annual screening, where workers were tested yearly; (2) targeted screening, where workers with high-risk duties (e.g. respiratory therapy) were tested yearly and other workers only after recognised exposure; and (3) post exposure-only screening, where all workers were tested only after recognised exposure. Workers with high-risk duties had 1% annual risk of infection, while workers with standard patient care duties had 0.3%. In an alternate higher-risk scenario, the corresponding annual risks of infection were 3% and 1%, respectively. We projected costs, morbidity, quality-adjusted survival and mortality over 20 years after hiring. The analysis used the healthcare system perspective and a 3% annual discount rate.
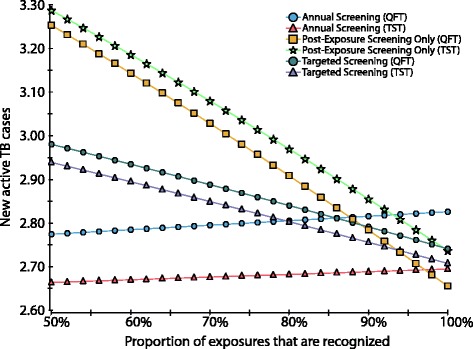
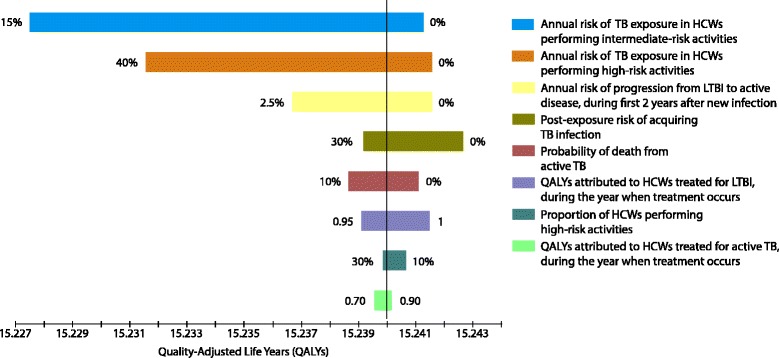
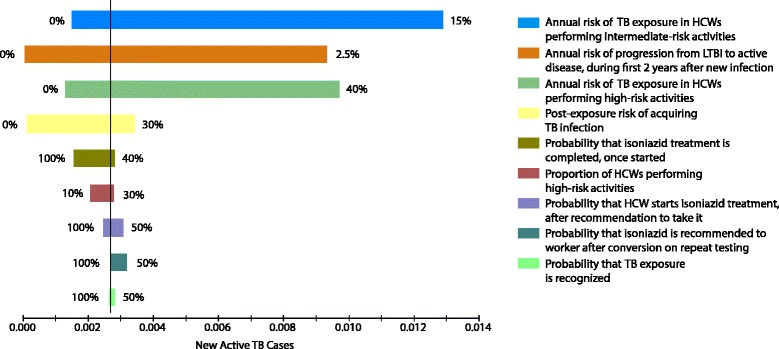
Over 20 years, annual screening with TST yielded an expected 2.68 active tuberculosis cases/1000 workers, versus 2.83 for targeted screening and 3.03 for post-exposure screening only. In all cases, annual screening was associated with poorer quality-adjusted survival, i.e. lost quality-adjusted life years, compared to targeted or post-exposure screening only. The annual TST screening strategy yielded an incremental cost estimate of $1,717,539 per additional case prevented versus targeted TST screening, which in turn cost an incremental $426,678 per additional case prevented versus post-exposure TST screening only. With the alternate "higher-risk" scenario, the annual TST strategy cost an estimated $426,678 per additional case prevented versus the targeted TST strategy, which cost an estimated $52,552 per additional case prevented versus post-exposure TST screening only. In all cases, QFT was more expensive than TST, with no or limited added benefit. Sensitivity analysis suggested that, even with limited exposure recognition, annual screening was poorly cost-effective.
For most North American healthcare workers, annual tuberculosis screening appears poorly cost-effective. Reconsideration of screening practices is warranted.
在北美,结核病发病率目前非常低,医护人员面临的风险已经下降。事实上,最近的队列数据对在这种情况下进行常规年度结核病筛查提出了质疑。我们比较了三种对有接触风险的北美医护人员进行持续筛查的潜在策略的成本效益。该分析未评估入职时筛查的成本效益,且仅考虑基线检测呈阴性的工作人员。
一个决策分析模型模拟了1000名基线检测呈阴性的工作人员的假设队列,考虑了工作职责、结核病接触情况、检测和治疗。对两种检测方法进行了建模,即结核菌素皮肤试验(TST)和全血γ干扰素释放试验(QFT)。比较了三种筛查策略:(1)年度筛查,即工作人员每年接受检测;(2)针对性筛查,即从事高风险工作(如呼吸治疗)的工作人员每年接受检测,其他工作人员仅在确认接触后接受检测;(3)仅接触后筛查,即所有工作人员仅在确认接触后接受检测。从事高风险工作的人员每年感染风险为1%,而从事标准患者护理工作的人员每年感染风险为0.3%。在另一种高风险情况下,相应的年度感染风险分别为3%和1%。我们预测了入职后20年的成本、发病率、质量调整生存期和死亡率。该分析采用医疗保健系统视角和3%的年度贴现率。
在20年期间,采用TST进行年度筛查,每1000名工作人员中预计有2.68例活动性结核病病例,针对性筛查为2.83例,仅接触后筛查为3.03例。在所有情况下,与仅进行针对性筛查或仅接触后筛查相比,年度筛查的质量调整生存期较差,即质量调整生命年损失。与针对性TST筛查相比,年度TST筛查策略每预防一例额外病例的增量成本估计为1,717,539美元,而针对性TST筛查与仅接触后TST筛查相比,每预防一例额外病例的增量成本为426,678美元。在另一种“高风险”情况下,年度TST策略每预防一例额外病例的成本估计为426,678美元,而针对性TST策略与仅接触后TST筛查相比,每预防一例额外病例的成本估计为52,552美元。在所有情况下,QFT比TST更昂贵,且没有或只有有限的额外益处。敏感性分析表明,即使接触确认有限,年度筛查的成本效益也很差。
对于大多数北美医护人员来说,年度结核病筛查的成本效益似乎很差。有必要重新考虑筛查做法。