University of Illinois at Chicago College of Medicine, Chicago, IL, USA.
Baylor College of Medicine, Houston, TX, USA.
Sex Med Rev. 2018 Jan;6(1):77-85. doi: 10.1016/j.sxmr.2017.04.001. Epub 2017 May 16.
A rapid increase in awareness of androgen deficiency has led to substantial increases in prescribing of testosterone therapy (TTh), with benefits of improvements in mood, libido, bone density, muscle mass, body composition, energy, and cognition. However, TTh can be limited by its side effects, particularly erythrocytosis. This review examines the literature on testosterone-induced erythrocytosis and polycythemia.
To review the available literature on testosterone-induced erythrocytosis, discuss possible mechanisms for pathophysiology, determine the significance of formulation, and elucidate potential thromboembolic risk.
A literature review was performed using PubMed for articles addressing TTh, erythrocytosis, and polycythemia.
Mechanism, pharmacologic contribution, and risk of testosterone-induced erythrocytosis.
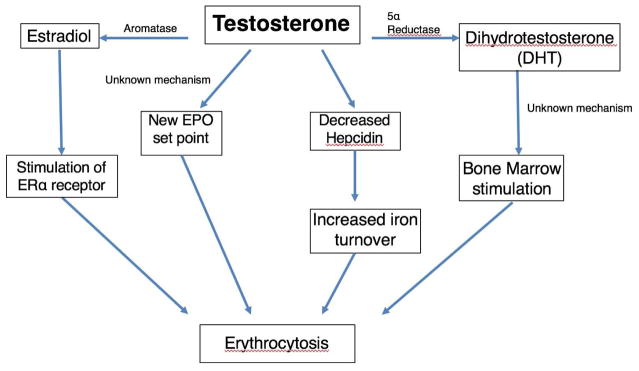
For men undergoing TTh, the risk of developing erythrocytosis compared with controls is well established, with short-acting injectable formulations having the highest associated incidence. Potential mechanisms explaining the relation between TTh and erythrocytosis include the role of hepcidin, iron sequestration and turnover, erythropoietin production, bone marrow stimulation, and genetic factors. High blood viscosity increases the risk for potential vascular complications involving the coronary, cerebrovascular, and peripheral vascular circulations, although there is limited evidence supporting a relation between TTh and vascular complications.
Short-acting injectable testosterone is associated with greater risk of erythrocytosis compared with other formulations. The mechanism of the pathophysiology and its role on thromboembolic events remain unclear, although some data support an increased risk of cardiovascular events resulting from testosterone-induced erythrocytosis. Ohlander SJ, Varghese B, Pastuszak AW. Erythrocytosis Following Testosterone Therapy. Sex Med Rev 2018;6:77-85.
雄激素缺乏症的认识迅速提高,导致睾酮治疗(TTh)的处方大量增加,其益处包括改善情绪、性欲、骨密度、肌肉量、身体成分、能量和认知。然而,TTh 可能会受到其副作用的限制,特别是红细胞增多症。本综述检查了关于睾酮引起的红细胞增多症和红细胞增多症的文献。
综述关于睾酮引起的红细胞增多症的现有文献,讨论可能的发病机制,确定配方的意义,并阐明潜在的血栓栓塞风险。
使用 PubMed 对涉及 TTh、红细胞增多症和红细胞增多症的文章进行文献复习。
机制、药物贡献和睾酮引起的红细胞增多症的风险。
对于接受 TTh 的男性,与对照组相比,发生红细胞增多症的风险已经得到很好的确立,短效注射制剂具有最高的相关发病率。解释 TTh 和红细胞增多症之间关系的潜在机制包括铁调素的作用、铁的隔离和周转、促红细胞生成素的产生、骨髓刺激和遗传因素。高血液黏度增加了涉及冠状动脉、脑血管和周围血管循环的潜在血管并发症的风险,尽管有有限的证据支持 TTh 和血管并发症之间的关系。
与其他制剂相比,短效注射用睾酮与红细胞增多症的风险增加有关。发病机制的机制及其在血栓栓塞事件中的作用尚不清楚,尽管一些数据支持由于睾酮引起的红细胞增多症导致心血管事件的风险增加。Ohlander SJ、Varghese B、Pastuszak AW。睾酮治疗后的红细胞增多症。性医学评论 2018;6:77-85。