Kiehl Erich L, Parker Alex M, Matar Ralph M, Gottbrecht Matthew F, Johansen Michelle C, Adams Mark P, Griffiths Lori A, Dunn Steven P, Bidwell Katherine L, Menon Venu, Enfield Kyle B, Gimple Lawrence W
Department of Cardiovascular Medicine, Cleveland Clinic Foundation, Cleveland, OH.
Department of Cardiovascular Medicine, University of Virginia, Charlottesville, VA.
J Am Heart Assoc. 2017 May 20;6(5):e003821. doi: 10.1161/JAHA.116.003821.
Out-of-hospital cardiac arrest (OHCA) results in significant morbidity and mortality, primarily from neurologic injury. Predicting neurologic outcome early post-OHCA remains difficult in patients receiving targeted temperature management.
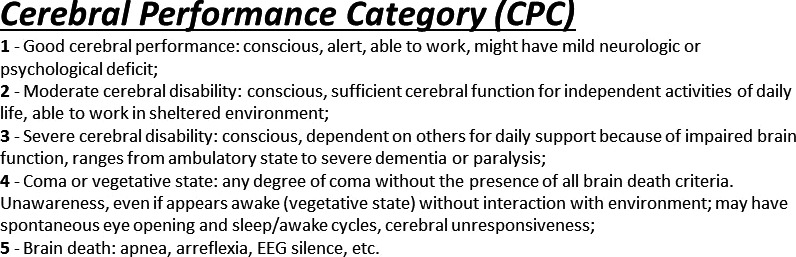
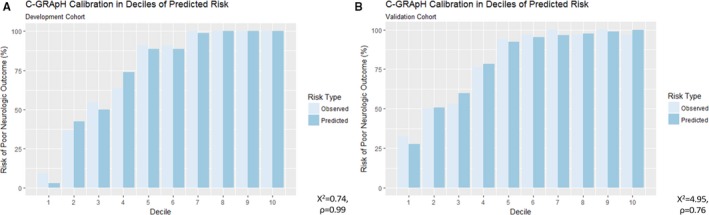
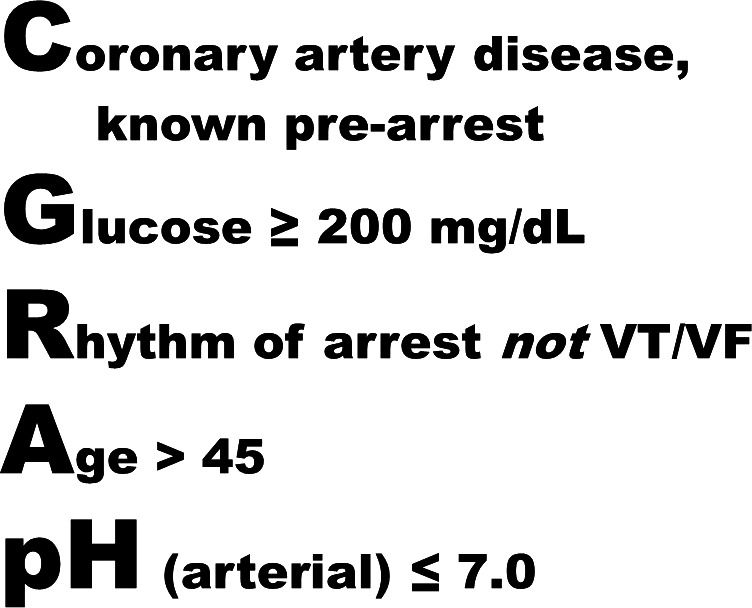
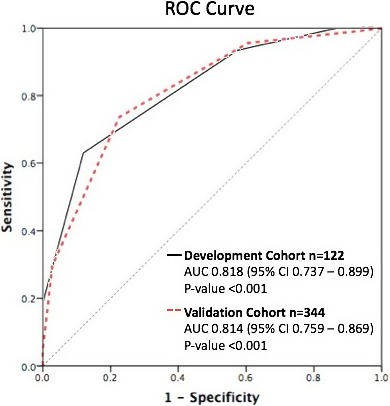
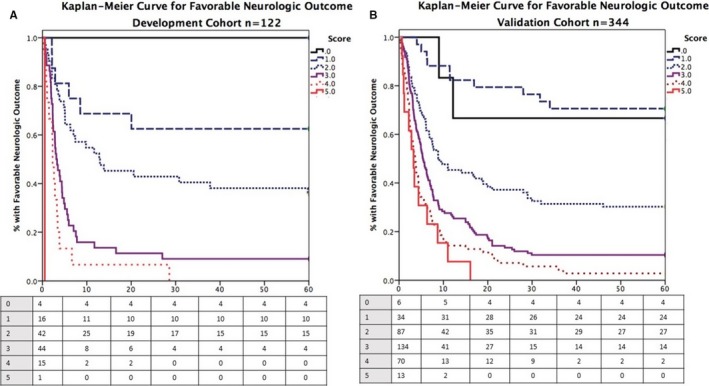
Retrospective analysis was performed on consecutive OHCA patients receiving targeted temperature management (32-34°C) for 24 hours at a tertiary-care center from 2008 to 2012 (development cohort, n=122). The primary outcome was favorable neurologic outcome at hospital discharge, defined as cerebral performance category 1 to 2 (poor 3-5). Patient demographics, pre-OHCA diagnoses, and initial laboratory studies post-resuscitation were compared between favorable and poor neurologic outcomes with multivariable logistic regression used to develop a simple scoring system (). The score ranges 0 to 5 using equally weighted variables: (): coronary artery disease, known pre-OHCA; (): glucose ≥200 mg/dL; (): rhythm of arrest not ventricular tachycardia/fibrillation; (): age >45; (): arterial pH ≤7.0. A validation cohort (n=344) included subsequent patients from the initial site (n=72) and an external quaternary-care health system (n=272) from 2012 to 2014. The c-statistic for predicting neurologic outcome was 0.82 (0.74-0.90, <0.001) in the development cohort and 0.81 (0.76-0.87, <0.001) in the validation cohort. When subdivided by score, similar rates of favorable neurologic outcome were seen in both cohorts, 70% each for low (0-1, n=60), 22% versus 19% for medium (2-3, n=307), and 0% versus 2% for high (4-5, n=99) scores in the development and validation cohorts, respectively.
stratifies neurologic outcomes following OHCA in patients receiving targeted temperature management (32-34°C) using objective data available at hospital presentation, identifying patient subsets with disproportionally favorable ( ≤1) and poor ( ≥4) prognoses.
院外心脏骤停(OHCA)会导致严重的发病率和死亡率,主要源于神经损伤。对于接受目标温度管理的患者,在OHCA后早期预测神经功能结局仍然困难。
对2008年至2012年在一家三级医疗中心连续接受目标温度管理(32 - 34°C)24小时的OHCA患者进行回顾性分析(开发队列,n = 122)。主要结局是出院时良好的神经功能结局,定义为脑功能分类1至2级(差为3至5级)。采用多变量逻辑回归分析比较了神经功能结局良好和不良患者的人口统计学特征、OHCA前诊断以及复苏后初始实验室检查结果,以建立一个简单的评分系统()。该评分使用等权重变量,范围为0至5分:():OHCA前已知冠状动脉疾病;():血糖≥200 mg/dL;():骤停节律不是室性心动过速/心室颤动;():年龄>45岁;():动脉pH≤7.0。验证队列(n = 344)包括2012年至2014年来自初始研究地点的后续患者(n = 72)和一个外部四级医疗保健系统的患者(n = 272)。在开发队列中,预测神经功能结局的c统计量为0.82(0.74 - 0.90,P<0.001),在验证队列中为0.81(0.76 - 0.87,P<0.001)。按评分细分时,两个队列中神经功能结局良好的发生率相似,开发队列和验证队列中低评分(0 - 1分,n = 60)的患者均为70%,中等评分(2 - 3分,n = 307)的患者分别为22%和19%,高评分(4 - 5分,n = 99)的患者分别为0%和2%。
使用入院时可用的客观数据对接受目标温度管理(32 - 34°C)的OHCA患者的神经功能结局进行分层,识别出预后差异较大的良好(评分≤1)和不良(评分≥4)患者亚组。