Fortune Brett, Cardenas Andres
Department of Gastroenterology and Hepatology, Weill Cornell Medical College, NY, USA.
Institut de Malalties Digestives i Metabolique, Hospital Clinic, University of Barcelona, Barcelona, Spain.
Gastroenterol Rep (Oxf). 2017 May;5(2):104-112. doi: 10.1093/gastro/gox010. Epub 2017 Apr 24.
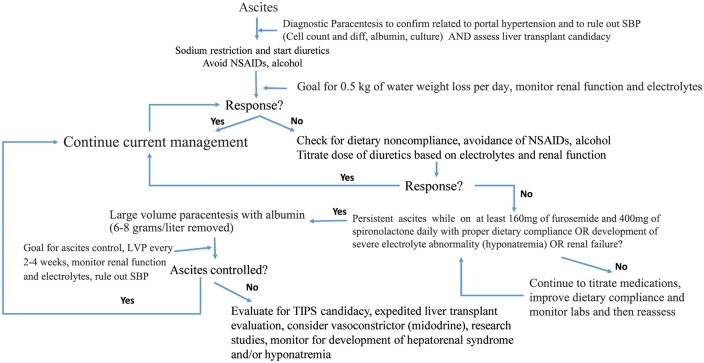
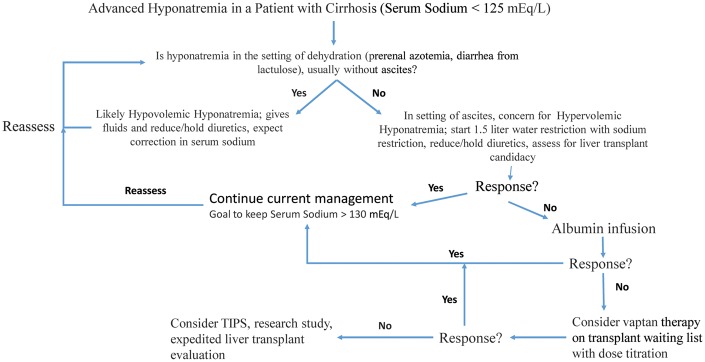
Ascites is the most common complication related to cirrhosis and is associated with increased morbidity and mortality. Ascites is a consequence of the loss of compensatory mechanisms to maintain the overall effective arterial blood volume due to worsening splanchnic arterial vasodilation as a result of clinically significant portal hypertension. In order to maintain effective arterial blood volume, vasoconstrictor and antinatriuretic pathways are activated, which increase overall sodium and fluid retention. As a result of progressive splanchnic arterial vasodilation, intestinal capillary pressure increases and results in the formation of protein-poor fluid within the abdominal cavity due to increased capillary permeability from the hepatic sinusoidal hypertension. In some patients, the fluid can translocate across diaphragmatic fenestrations into the pleural space, leading to hepatic hydrothorax. In addition, infectious complications such as spontaneous bacterial peritonitis can occur. Eventually, as the liver disease progresses related to higher portal pressures, loss of a compensatory cardiac output and further splanchnic vasodilation, kidney function becomes compromised from worsening renal vasoconstriction as well as the development of impaired solute-free water excretion and severe sodium retention. These mechanisms then translate into significant clinical complications, such as refractory ascites, hepatorenal syndrome and hyponatremia, and all are linked to increased short-term mortality. Currently, liver transplantation is the only curative option for this spectrum of clinical manifestations but ongoing research has led to further insight on alternative approaches. This review will further explore the current understanding on the pathophysiology and management of ascites as well as expand on two advanced clinical consequences of advanced liver disease, refractory ascites and hyponatremia.
腹水是肝硬化最常见的并发症,与发病率和死亡率的增加相关。腹水是由于临床上显著的门静脉高压导致内脏动脉血管舒张恶化,维持总体有效动脉血容量的代偿机制丧失的结果。为了维持有效动脉血容量,血管收缩和抗利尿途径被激活,这增加了总体钠和液体潴留。由于内脏动脉逐渐舒张,肠毛细血管压力增加,由于肝窦高压导致毛细血管通透性增加,从而在腹腔内形成蛋白含量低的液体。在一些患者中,液体可通过膈肌小孔转移至胸腔,导致肝性胸水。此外,还可能发生自发性细菌性腹膜炎等感染性并发症。最终,随着与更高门静脉压力相关的肝脏疾病进展、代偿性心输出量丧失以及进一步的内脏血管舒张,肾功能因肾血管收缩恶化、无溶质自由水排泄受损和严重钠潴留的发展而受损。这些机制进而转化为严重的临床并发症,如难治性腹水、肝肾综合征和低钠血症,所有这些都与短期死亡率增加有关。目前,肝移植是针对这一系列临床表现的唯一治愈选择,但正在进行的研究已带来对替代方法的进一步认识。本综述将进一步探讨目前对腹水病理生理学和管理的理解,并详述晚期肝病的两个严重临床后果,即难治性腹水和低钠血症。