Sukul Devraj, Seth Milan, Schreiber Theodore, Hanzel George, Khandelwal Akshay, Cannon Louis A, Lalonde Thomas A, Gurm Hitinder S
Department of Internal Medicine, Division of Cardiovascular Medicine, University of Michigan, Ann Arbor, Michigan.
Detroit Medical Center-Cardiovascular Institute, Detroit, Michigan.
J Interv Cardiol. 2017 Aug;30(4):291-300. doi: 10.1111/joic.12388. Epub 2017 May 22.
We sought to evaluate the patterns of use and outcomes associated with eptifibatide and abciximab administration among dialysis patients who underwent percutaneous coronary intervention (PCI).
Contraindicated medications are frequently administered to dialysis patients undergoing PCI often resulting in adverse outcomes. Eptifibatide is a glycoprotein IIb/IIIa inhibitor that is often used during PCI and is contraindicated in dialysis.
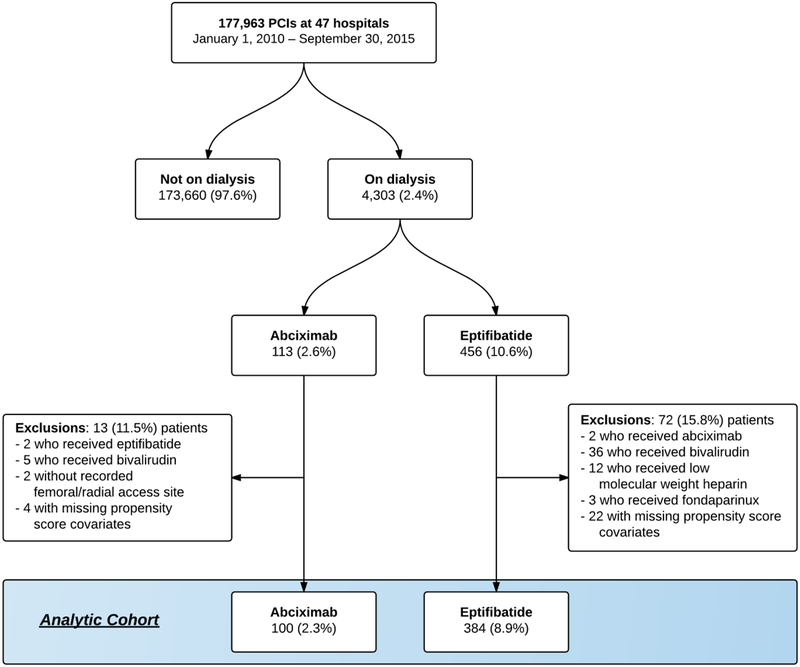
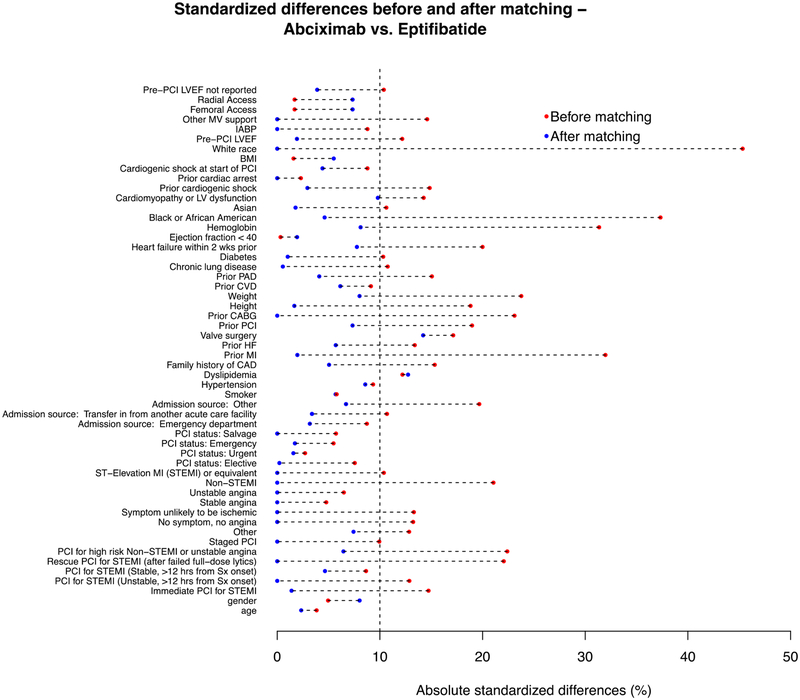
We included dialysis patients who underwent PCI from January 2010 to September 2015 at 47 hospitals in Michigan. We compared outcomes between patients who received eptifibatide compared with abciximab. Both groups required concurrent treatment with unfractionated heparin only. In-hospital outcomes included repeat PCI, bleeding, major bleeding, need for transfusion, and death. Optimal full matching was used to adjust for non-random drug administration.
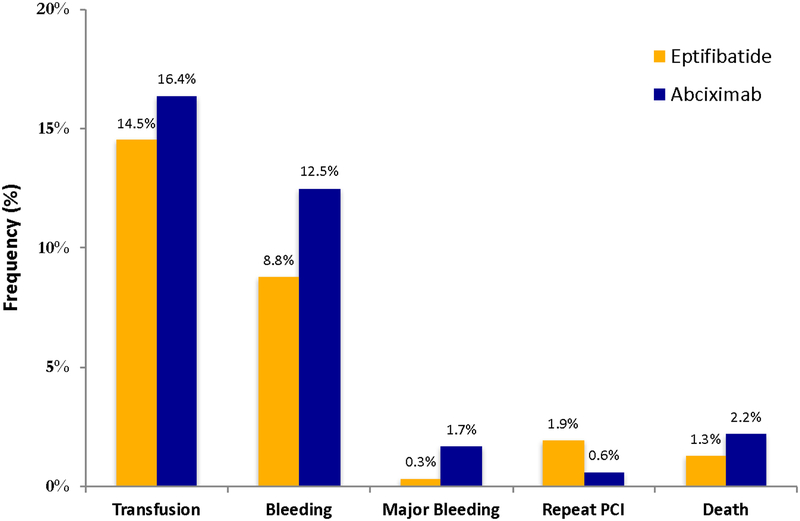
Of 177 963 patients who underwent PCI, 4303 (2.4%) were on dialysis. Among those, 384 (8.9%) received eptifibatide and 100 (2.3%) received abciximab. Prior to matching, patients who received eptifibatide had higher pre-procedural hemoglobin levels (11.3 g/dL vs. 10.7 g/dL; P < 0.001) and less frequently had a history of myocardial infarction (36.5% vs. 52.0%; P = 0.005). After matching, there were no significant differences in in-hospital outcomes between eptifibatide and abciximab including transfusion (aOR: 1.15; 95%CI: 0.55-2.40; P = 0.70), bleeding (1.47; 0.64-3.40; P = 0.36), major bleeding (4.68; 0.42-52.3; P = 0.21), repeat PCI (0.38; 0.03-4.23; P = 0.43), and death (1.53; 0.2-9.05; P = 0.64).
Despite being contraindicated in dialysis, eptifibatide was used approximately 3.5 times more frequently than abciximab among dialysis patients undergoing PCI but was associated with similar in-hospital outcomes.
我们旨在评估接受经皮冠状动脉介入治疗(PCI)的透析患者使用依替巴肽和阿昔单抗的模式及相关结果。
禁忌药物经常被用于接受PCI的透析患者,这常常导致不良后果。依替巴肽是一种糖蛋白IIb/IIIa抑制剂,常用于PCI期间,但在透析患者中属于禁忌。
我们纳入了2010年1月至2015年9月期间在密歇根州47家医院接受PCI的透析患者。我们比较了接受依替巴肽与接受阿昔单抗的患者的结局。两组均仅需同时使用普通肝素进行治疗。住院期间的结局包括再次PCI、出血、大出血、输血需求和死亡。采用最优完全匹配法对非随机药物使用情况进行调整。
在177963例接受PCI的患者中,4303例(2.4%)为透析患者。其中,384例(8.9%)接受了依替巴肽治疗,100例(2.3%)接受了阿昔单抗治疗。在匹配前,接受依替巴肽治疗的患者术前血红蛋白水平较高(11.3g/dL对10.7g/dL;P<0.001),心肌梗死病史的发生率较低(36.5%对52.0%;P=0.005)。匹配后,依替巴肽组和阿昔单抗组在住院结局方面无显著差异,包括输血(调整后比值比:1.15;95%置信区间:0.55-2.40;P=0.70)、出血(1.47;0.64-3.40;P=0.36)、大出血(4.68;0.42-52.3;P=0.21)、再次PCI(0.38;0.03-4.23;P=0.43)和死亡(1.53;0.2-9.05;P=0.64)。
尽管依替巴肽在透析患者中属禁忌,但在接受PCI的透析患者中,其使用频率约为阿昔单抗的3.5倍,不过二者的住院结局相似。