Moreira Sandra, Wood Libby, Smith Debbie, Marini-Bettolo Chiara, Guglieri Michela, McMacken Grace, Bailey Geraldine, Mayhew Anna, Muni-Lofra Robert, Eglon Gail, Williams Maggie, Straub Volker, Lochmüller Hanns, Evangelista Teresinha
Serviço de Neurologia, Centro Hospitalar Entre Douro e Vouga, Santa Maria da Feira, Portugal.
John Walton Muscular Dystrophy Research Centre, MRC Centre for Neuromuscular Diseases, Institute of Genetic Medicine, Newcastle University, Central Parkway, Newcastle upon Tyne, NE1 3BZ, UK.
J Neurol. 2017 Jun;264(6):1271-1280. doi: 10.1007/s00415-017-8525-9. Epub 2017 May 26.
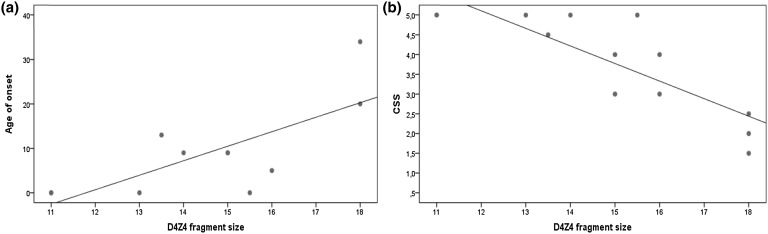
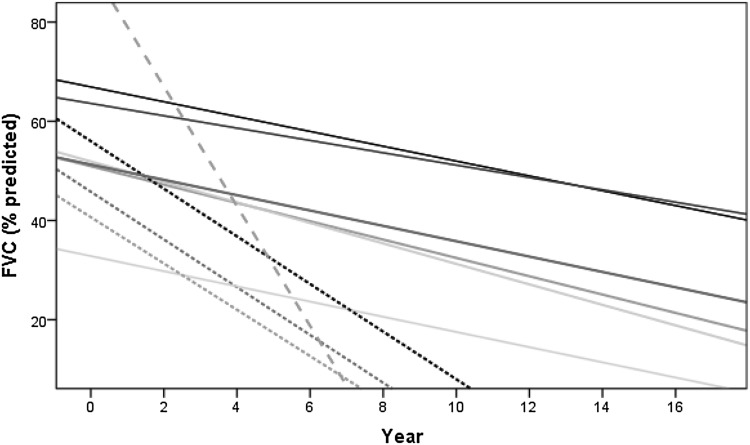
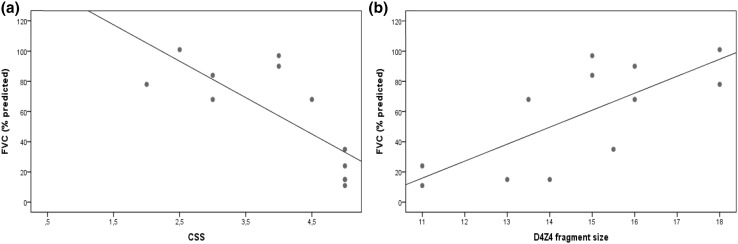
Understand the occurrence and predictors of respiratory impairment in FSHD. Data from 100 FSHD patients was collected regarding demographics, genetics, respiratory status and pulmonary function tests, clinical manifestations and Clinical Severity Scale (CSS) scores. Patients were assigned to two severity groups using CSS: mild (scores <3.5) and moderate/severely affected (scores ≥3.5). Forced Vital Capacity (FVC) was classified as severely impaired if less than 50% of the predicted. Statistical analysis was performed using IBM SPSS Statistics 23, tests were two-tailed and the level of significance set at 5%. Spirometry was available for 94 patients; 41.5% had abnormal results with a restrictive pattern in 38.3% patients. There was a correlation between FVC; CSS score and D4Z4 fragment length with a higher probability of severe respiratory involvement in the early onset group, moderate/severe disease and D4Z4 fragments <18 kb. Patients with severe respiratory involvement showed a high prevalence of sleep-disordered breathing. FVC decline over time was indicative of three progression groups. Respiratory involvement for both ambulant and non-ambulant patients with FSHD is more frequent and severe than previously suggested. Sleep-disordered breathing is frequent and negatively influences the respiratory status. Annual screening of the respiratory status with spirometry and clinical assessment is thus warranted in FSHD patients, even while ambulant.
了解面肩肱型肌营养不良症(FSHD)中呼吸功能损害的发生情况及预测因素。收集了100例FSHD患者的人口统计学、遗传学、呼吸状况、肺功能测试、临床表现及临床严重程度量表(CSS)评分等数据。使用CSS将患者分为两个严重程度组:轻度(评分<3.5)和中度/重度受累(评分≥3.5)。如果用力肺活量(FVC)低于预测值的50%,则被分类为严重受损。使用IBM SPSS Statistics 23进行统计分析,检验为双侧检验,显著性水平设定为5%。94例患者进行了肺活量测定;41.5%的结果异常,其中38.3%的患者呈现限制性模式。FVC、CSS评分与D4Z4片段长度之间存在相关性,早发型组、中度/重度疾病以及D4Z4片段<18 kb的患者发生严重呼吸受累的可能性更高。严重呼吸受累的患者睡眠呼吸障碍患病率较高。FVC随时间的下降表明存在三个进展组。FSHD的行走和非行走患者的呼吸受累比之前认为的更频繁、更严重。睡眠呼吸障碍很常见,且对呼吸状况有负面影响。因此,即使是行走的FSHD患者,也有必要每年通过肺活量测定和临床评估对呼吸状况进行筛查。