Snyder Alexandra, Nathanson Tavi, Funt Samuel A, Ahuja Arun, Buros Novik Jacqueline, Hellmann Matthew D, Chang Eliza, Aksoy Bulent Arman, Al-Ahmadie Hikmat, Yusko Erik, Vignali Marissa, Benzeno Sharon, Boyd Mariel, Moran Meredith, Iyer Gopa, Robins Harlan S, Mardis Elaine R, Merghoub Taha, Hammerbacher Jeff, Rosenberg Jonathan E, Bajorin Dean F
Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York, United States of America.
Department of Medicine, Weill Cornell Medical College, New York, New York, United States of America.
PLoS Med. 2017 May 26;14(5):e1002309. doi: 10.1371/journal.pmed.1002309. eCollection 2017 May.
Inhibition of programmed death-ligand 1 (PD-L1) with atezolizumab can induce durable clinical benefit (DCB) in patients with metastatic urothelial cancers, including complete remissions in patients with chemotherapy refractory disease. Although mutation load and PD-L1 immune cell (IC) staining have been associated with response, they lack sufficient sensitivity and specificity for clinical use. Thus, there is a need to evaluate the peripheral blood immune environment and to conduct detailed analyses of mutation load, predicted neoantigens, and immune cellular infiltration in tumors to enhance our understanding of the biologic underpinnings of response and resistance.
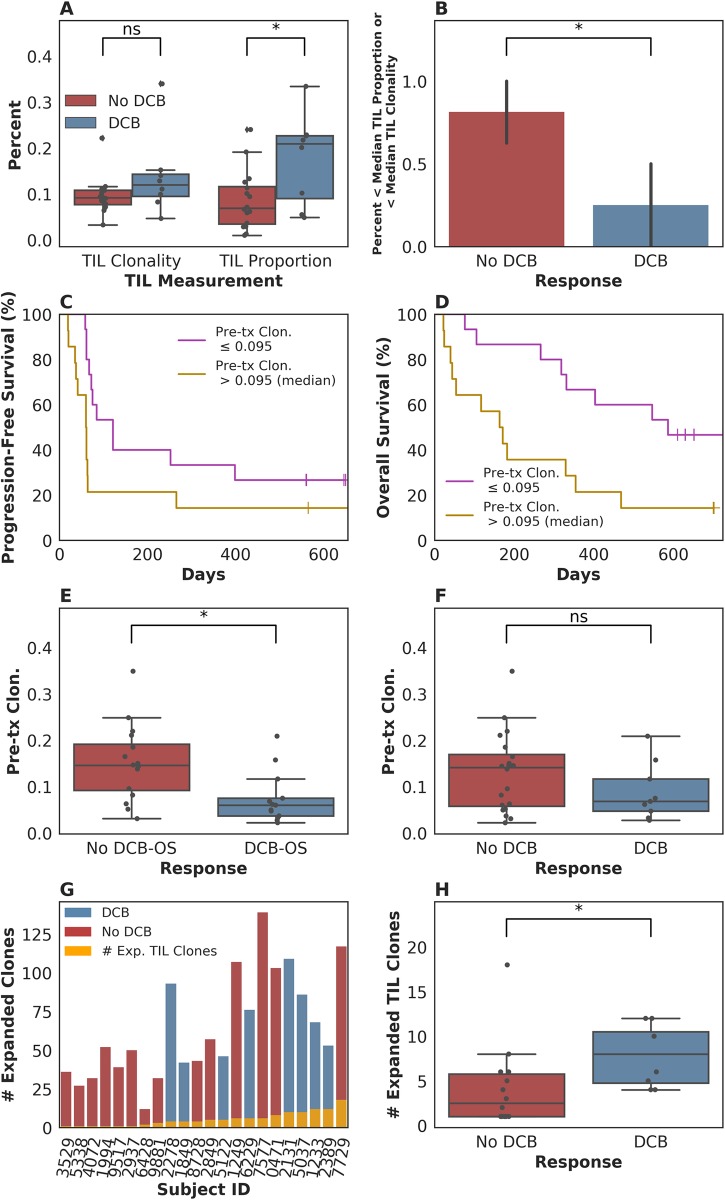
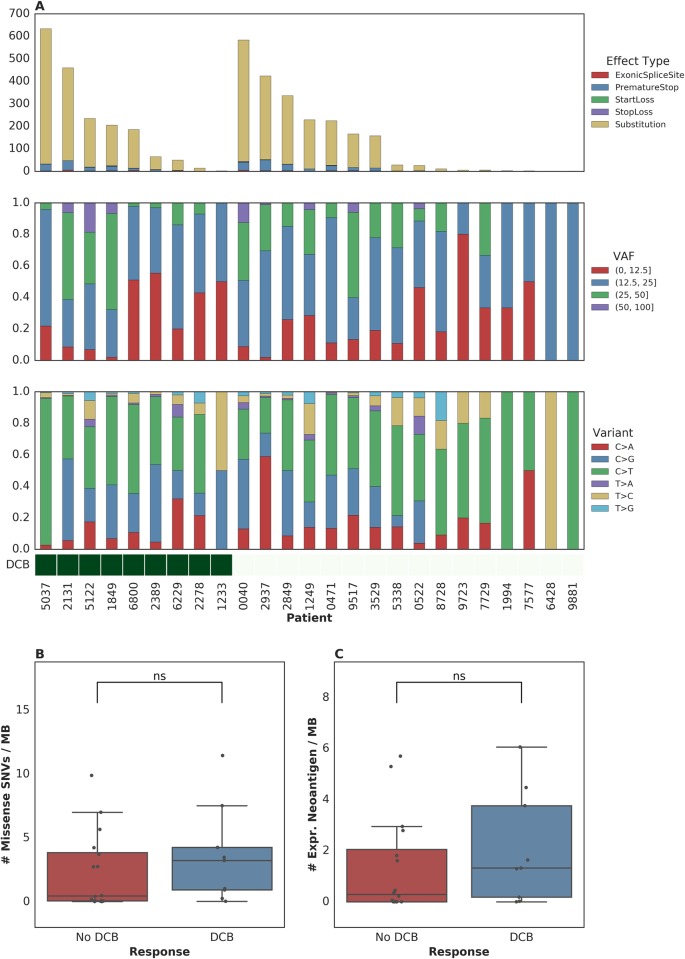
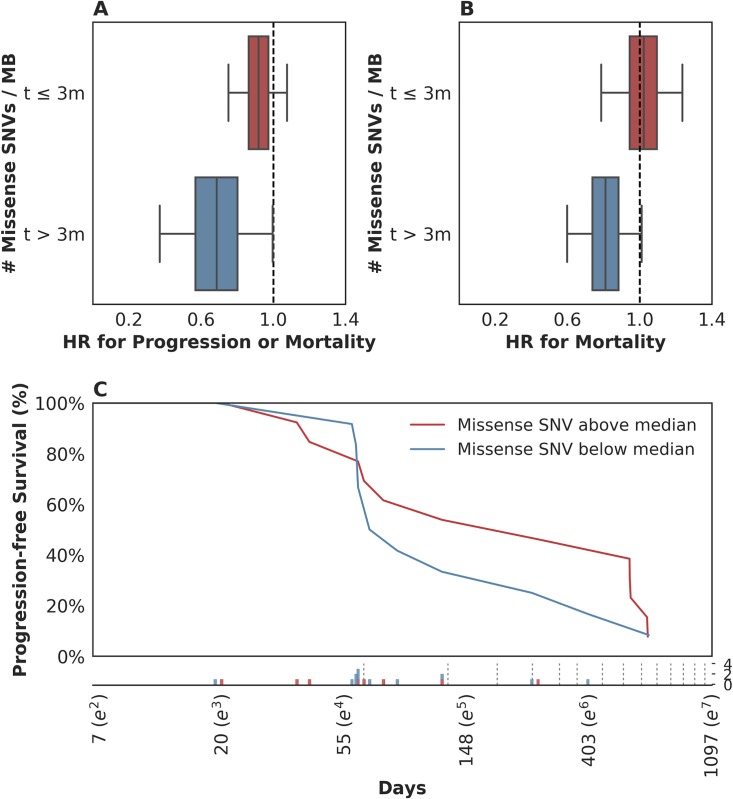
The goals of this study were to (1) evaluate the association of mutation load and predicted neoantigen load with therapeutic benefit and (2) determine whether intratumoral and peripheral blood T cell receptor (TCR) clonality inform clinical outcomes in urothelial carcinoma treated with atezolizumab. We hypothesized that an elevated mutation load in combination with T cell clonal dominance among intratumoral lymphocytes prior to treatment or among peripheral T cells after treatment would be associated with effective tumor control upon treatment with anti-PD-L1 therapy. We performed whole exome sequencing (WES), RNA sequencing (RNA-seq), and T cell receptor sequencing (TCR-seq) of pretreatment tumor samples as well as TCR-seq of matched, serially collected peripheral blood, collected before and after treatment with atezolizumab. These parameters were assessed for correlation with DCB (defined as progression-free survival [PFS] >6 months), PFS, and overall survival (OS), both alone and in the context of clinical and intratumoral parameters known to be predictive of survival in this disease state. Patients with DCB displayed a higher proportion of tumor-infiltrating T lymphocytes (TIL) (n = 24, Mann-Whitney p = 0.047). Pretreatment peripheral blood TCR clonality below the median was associated with improved PFS (n = 29, log-rank p = 0.048) and OS (n = 29, log-rank p = 0.011). Patients with DCB also demonstrated more substantial expansion of tumor-associated TCR clones in the peripheral blood 3 weeks after starting treatment (n = 22, Mann-Whitney p = 0.022). The combination of high pretreatment peripheral blood TCR clonality with elevated PD-L1 IC staining in tumor tissue was strongly associated with poor clinical outcomes (n = 10, hazard ratio (HR) (mean) = 89.88, HR (median) = 23.41, 95% CI [2.43, 506.94], p(HR > 1) = 0.0014). Marked variations in mutation loads were seen with different somatic variant calling methodologies, which, in turn, impacted associations with clinical outcomes. Missense mutation load, predicted neoantigen load, and expressed neoantigen load did not demonstrate significant association with DCB (n = 25, Mann-Whitney p = 0.22, n = 25, Mann-Whitney p = 0.55, and n = 25, Mann-Whitney p = 0.29, respectively). Instead, we found evidence of time-varying effects of somatic mutation load on PFS in this cohort (n = 25, p = 0.044). A limitation of our study is its small sample size (n = 29), a subset of the patients treated on IMvigor 210 (NCT02108652). Given the number of exploratory analyses performed, we intend for these results to be hypothesis-generating.
These results demonstrate the complex nature of immune response to checkpoint blockade and the compelling need for greater interrogation and data integration of both host and tumor factors. Incorporating these variables in prospective studies will facilitate identification and treatment of resistant patients.
阿替利珠单抗抑制程序性死亡配体1(PD-L1)可使转移性尿路上皮癌患者获得持久临床获益(DCB),包括化疗难治性疾病患者的完全缓解。尽管突变负荷和PD-L1免疫细胞(IC)染色与反应相关,但它们在临床应用中缺乏足够的敏感性和特异性。因此,有必要评估外周血免疫环境,并对肿瘤中的突变负荷、预测的新抗原和免疫细胞浸润进行详细分析,以加深我们对反应和耐药生物学基础的理解。
本研究的目的是(1)评估突变负荷和预测的新抗原负荷与治疗获益的相关性,以及(2)确定肿瘤内和外周血T细胞受体(TCR)克隆性是否能为接受阿替利珠单抗治疗的尿路上皮癌患者的临床结局提供信息。我们假设,治疗前肿瘤内淋巴细胞或治疗后外周T细胞中突变负荷升高与T细胞克隆优势相结合,将与抗PD-L1治疗后的有效肿瘤控制相关。我们对治疗前肿瘤样本进行了全外显子组测序(WES)、RNA测序(RNA-seq)和T细胞受体测序(TCR-seq),以及在阿替利珠单抗治疗前后匹配的、连续收集的外周血的TCR-seq。评估这些参数与DCB(定义为无进展生存期[PFS]>6个月)、PFS和总生存期(OS)的相关性,单独评估以及结合已知可预测该疾病状态下生存的临床和肿瘤内参数进行评估。有DCB的患者显示肿瘤浸润性T淋巴细胞(TIL)比例更高(n = 24,Mann-Whitney p = 0.047)。治疗前外周血TCR克隆性低于中位数与PFS改善(n = 29,log-rank p = 0.048)和OS改善(n = 29,log-rank p = 0.011)相关。有DCB的患者在开始治疗3周后外周血中肿瘤相关TCR克隆也有更显著的扩增(n = 22,Mann-Whitney p = 0.022)。治疗前外周血TCR克隆性高与肿瘤组织中PD-L1 IC染色升高相结合与不良临床结局密切相关(n = 10,风险比(HR)(均值)= 89.88,HR(中位数)= 23.41,95% CI [2.43, 506.94],p(HR > 1) = 0.0014)。不同的体细胞变异检测方法导致突变负荷有显著差异,这反过来又影响了与临床结局的关联。错义突变负荷、预测的新抗原负荷和表达的新抗原负荷与DCB无显著关联(分别为n = 25,Mann-Whitney p = 0.22;n = 25,Mann-Whitney p = 0.55;n = 25,Mann-Whitney p = 0.29)。相反,我们在该队列中发现了体细胞突变负荷对PFS的时变效应证据(n = 25,p = 0.044)。我们研究的一个局限性是样本量小(n = 29),是在IMvigor 210(NCT02108652)上治疗的患者的一个子集。鉴于进行的探索性分析数量,我们希望这些结果能产生假设。
这些结果证明了对检查点阻断免疫反应的复杂性,以及迫切需要对宿主和肿瘤因素进行更深入的研究和数据整合。将这些变量纳入前瞻性研究将有助于识别和治疗耐药患者。