Halpern A B, Othus M, Huebner E M, Buckley S A, Pogosova-Agadjanyan E L, Orlowski K F, Scott B L, Becker P S, Hendrie P C, Chen T L, Percival M-E M, Estey E H, Stirewalt D L, Walter R B
Clinical Research Division, Fred Hutchinson Cancer Research Center, Seattle, WA, USA.
Division of Hematology/Department of Medicine, University of Washington, Seattle, WA, USA.
Leukemia. 2017 Dec;31(12):2560-2567. doi: 10.1038/leu.2017.165. Epub 2017 May 30.
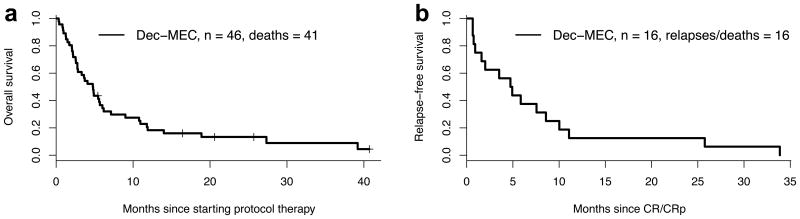
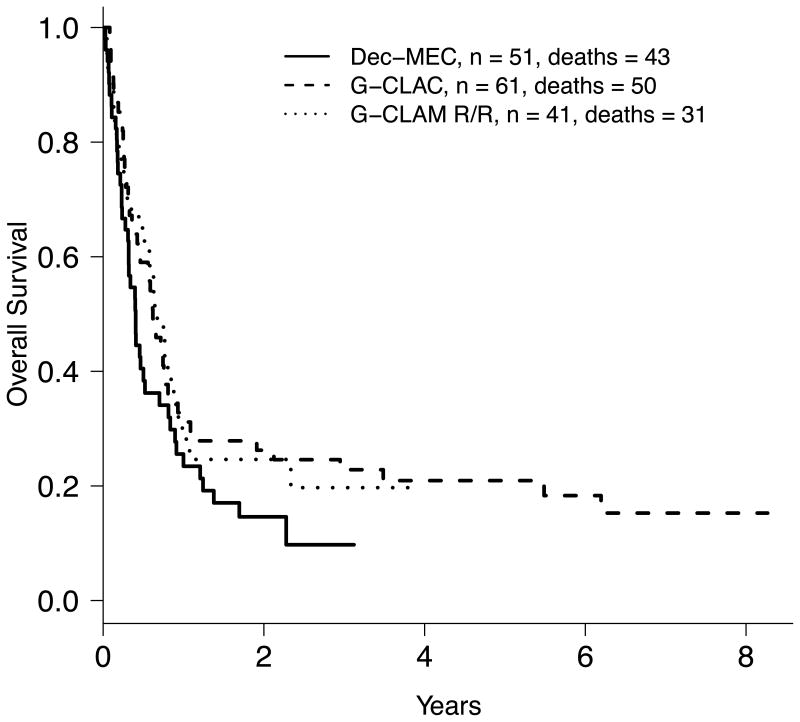
DNA methyltransferase inhibitors sensitize leukemia cells to chemotherapeutics. We therefore conducted a phase 1/2 study of mitoxantrone, etoposide and cytarabine following 'priming' with 5-10 days of decitabine (dec/MEC) in 52 adults (median age 55 (range: 19-72) years) with relapsed/refractory acute myeloid leukemia (AML) or other high-grade myeloid neoplasms. During dose escalation in cohorts of 6-12 patients, all dose levels were well tolerated. As response rates appeared similar with 7 and 10 days of decitabine, a 7-day course was defined as the recommended phase 2 dose (RP2D). Among 46 patients treated at/above the RP2D, 10 (22%) achieved a complete remission (CR), 8 without measurable residual disease; five additional patients achieved CR with incomplete platelet recovery, for an overall response rate of 33%. Seven patients (15%) died within 28 days of treatment initiation. Infection/neutropenic fever, nausea and mucositis were the most common adverse events. While the CR rate compared favorably to a matched historic control population (observed/expected CR ratio=1.77), CR rate and survival were similar to two contemporary salvage regimens used at our institution (G-CLAC (granulocyte colony-stimulating factor (G-CSF); clofarabine; cytarabine) and G-CLAM (G-CSF; cladribine; cytarabine; mitoxantrone)). Thus, while meeting the prespecified efficacy goal, we found no evidence that dec/MEC is substantially better than other cytarabine-based regimens currently used for relapsed/refractory AML.
DNA甲基转移酶抑制剂可使白血病细胞对化疗药物敏感。因此,我们对52名成年患者(中位年龄55岁(范围:19 - 72岁))进行了一项1/2期研究,这些患者患有复发/难治性急性髓系白血病(AML)或其他高级别髓系肿瘤,在使用地西他滨进行5 - 10天的“预处理”(地西他滨/米托蒽醌、依托泊苷和阿糖胞苷)后接受米托蒽醌、依托泊苷和阿糖胞苷治疗。在6 - 12名患者的队列中进行剂量递增时,所有剂量水平的耐受性都良好。由于地西他滨7天和10天的治疗方案的缓解率似乎相似,因此确定7天疗程为推荐的2期剂量(RP2D)。在46名接受RP2D及以上剂量治疗的患者中,10名(22%)实现了完全缓解(CR),其中8名无可测量的残留疾病;另外5名患者实现了血小板恢复不完全的CR,总缓解率为33%。7名患者(15%)在治疗开始后28天内死亡。感染/中性粒细胞减少性发热、恶心和粘膜炎是最常见的不良事件。虽然CR率与匹配的历史对照人群相比具有优势(观察到的/预期的CR比率 = 1.77),但CR率和生存率与我们机构使用的两种当代挽救方案(G - CLAC(粒细胞集落刺激因子(G - CSF);氯法拉滨;阿糖胞苷)和G - CLAM(G - CSF;克拉屈滨;阿糖胞苷;米托蒽醌))相似。因此,虽然达到了预先设定的疗效目标,但我们没有发现证据表明地西他滨/米托蒽醌、依托泊苷和阿糖胞苷方案比目前用于复发/难治性AML的其他基于阿糖胞苷的方案有显著更好的效果。