Kyaw Nang Thu Thu, Kumar Ajay M V, Oo Myo Minn, Oo Htun Nyunt, Kyaw Khine Wut Yee, Thiha Soe, Aung Thet Ko, Win Than, Mon Yin Yin, Harries Anthony D
a The Union Office in Myanmar , International Union Against Tuberculosis and Lung Disease , Mandalay , Myanmar.
b The Union South-East Asia Regional Office , International Union Against Tuberculosis and Lung Disease , New Delhi , India.
Glob Health Action. 2017;10(1):1290916. doi: 10.1080/16549716.2017.1290916.
Myanmar has a high burden of Human Immunodeficiency Virus (HIV) and second-line antiretroviral treatment (ART) has been available since 2008 in the public health sector. However, there have been no published data about the outcomes of such patients until now.
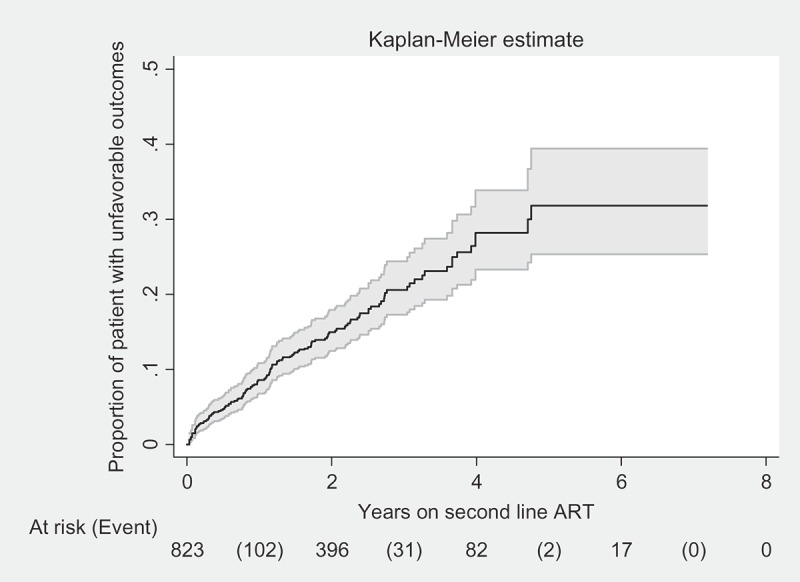
To assess the treatment and programmatic outcomes and factors associated with unfavorable outcomes (treatment failure, death and loss to follow-up from care) among people living with HIV (aged ≥ 10 years) receiving protease inhibitor-based second-line ART under the Integrated HIV Care Program in Myanmar between October 2008 and June 2015.
Retrospective cohort study using routinely collected program data.
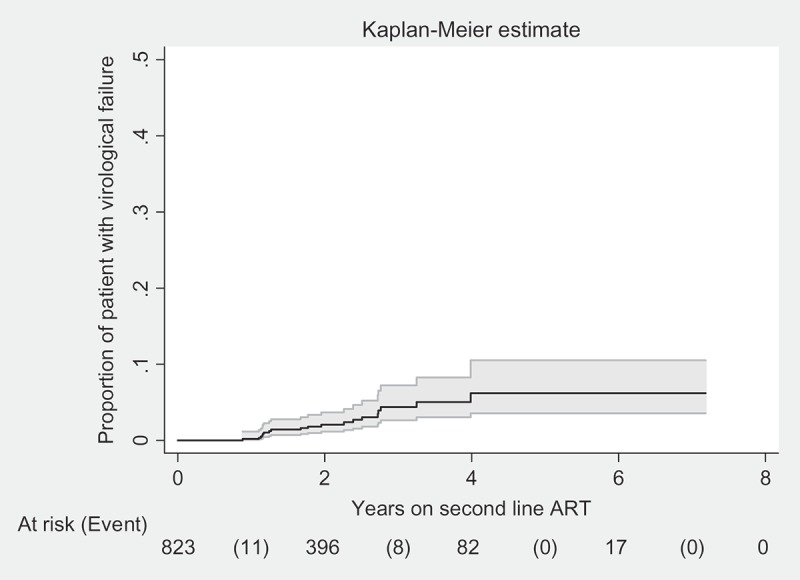
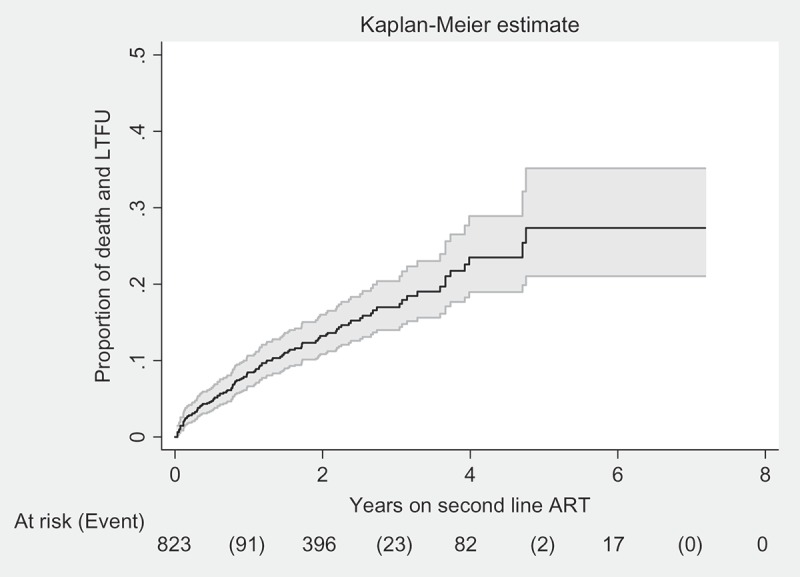
Of 824 adults and adolescents on second-line ART, 52 patients received viral load testing and 19 patients were diagnosed with virological failure. However, their treatment was not modified. At the end of a total follow-up duration of 7 years, 88 (11%) patients died, 35 (4%) were lost to follow-up, 21 (2%) were transferred out to other health facilities and 680 (83%) were still under care. The incidence rate of unfavorable outcomes was 7.9 patients per 100 person years follow-up. Patients with a history of injecting drug use, with a history of lost to follow-up, with a higher baseline viral load and who had received didanosine and abacavir had a higher risk of unfavorable outcomes. Patients with higher baseline C4 counts, those having taken first-line ART at a private clinic, receiving ART at decentralized sites and taking zidovudine and lamivudine had a lower risk of unfavorable outcomes.
Long-term outcomes of patients on second-line ART were relatively good in this cohort. Virological failure was relatively low, possibly because of lack of viral load testing. No patient who failed on second-line ART was switched to third-line treatment. The National HIV/AIDS Program should consider making routine viral load monitoring and third-line ART drugs available after a careful cost-benefit analysis.
缅甸的人类免疫缺陷病毒(HIV)负担沉重,自2008年起公共卫生部门就已提供二线抗逆转录病毒治疗(ART)。然而,迄今为止尚无关于此类患者治疗结果的公开数据。
评估2008年10月至2015年6月期间在缅甸综合HIV护理项目下接受基于蛋白酶抑制剂的二线ART治疗的HIV感染者(年龄≥10岁)的治疗及项目结局,以及与不良结局(治疗失败、死亡和失访)相关的因素。
采用常规收集的项目数据进行回顾性队列研究。
在824例接受二线ART治疗的成人和青少年中,52例患者接受了病毒载量检测,19例被诊断为病毒学失败。然而,他们的治疗方案并未调整。在总共7年的随访期结束时,88例(11%)患者死亡,35例(4%)失访,21例(2%)转至其他医疗机构,680例(83%)仍在接受治疗。不良结局的发生率为每100人年随访7.9例患者。有注射吸毒史、有失访史、基线病毒载量较高以及接受过去羟肌苷和阿巴卡韦治疗的患者出现不良结局的风险较高。基线C4细胞计数较高、在私人诊所接受过一线ART治疗、在分散地点接受ART治疗以及接受齐多夫定和拉米夫定治疗的患者出现不良结局的风险较低。
该队列中接受二线ART治疗患者的长期结局相对较好。病毒学失败率相对较低,可能是因为缺乏病毒载量检测。没有二线ART治疗失败的患者转换为三线治疗。国家HIV/AIDS项目应在仔细进行成本效益分析后考虑提供常规病毒载量监测和三线ART药物。