Bankova Andriyana, Andres Yvonne, Horn Michael P, Alberio Lorenzo, Nagler Michael
Division of Haematology and Central Haematology Laboratory, Luzerner Kantonsspital, Lucerne, Switzerland.
Kreisspital für das Freiamt, Muri, Switzerland.
PLoS One. 2017 Jun 8;12(6):e0178289. doi: 10.1371/journal.pone.0178289. eCollection 2017.
Immunoassays are crucial in the work-up of patients with suspected heparin-induced thrombocytopenia (HIT) and rapid tests have been recently developed. However, comparative data on diagnostic accuracy, reproducibility, and analytical costs of different immunoassays in clinical practice are limited.
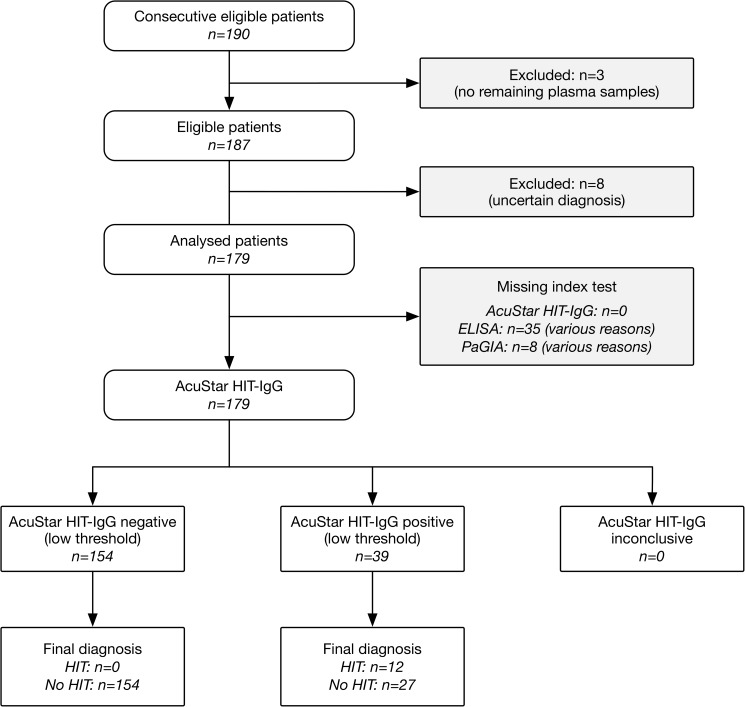
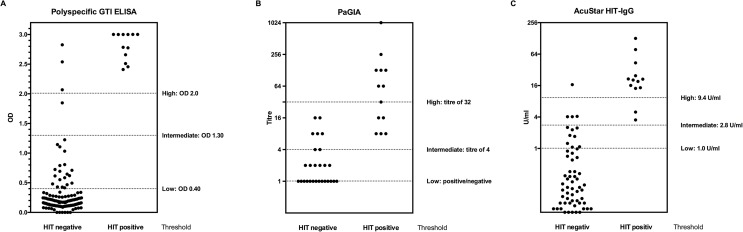
Samples of 179 consecutive patients evaluated for suspected HIT in clinical practice using a polyspecific enzyme-linked immunoabsorbent assay (GTI diagnostics; ELISA) and a rapid particle gel immunoassay (PaGIA), were additionally analysed with a IgG-specific chemiluminescent immunoassay (AcuStar HIT-IgG). Presence of HIT was defined as a positive functional heparin-induced platelet aggregation test. Diagnostic accuracy was determined for low, intermediate and high thresholds as previously established (ELISA: optical density 0.4, 1.3, and 2.0 respectively; PaGIA: positive/negative, titre of 4, titre of 32; AcuStar HIT-IgG: 1.0 U/ml, 2.8, 9.4) and reproducibility was assessed by repeated measurements. Costs of test determination were calculated taking reagents, controls, and working time of technicians according to Swiss health care system into account.
Data on PaGIA results were available for 171 patients (95.5%), ELISA for 144 patients (80.4%), and AcuStar HIT-IgG for 179 patients (100%). Sensitivity was above 95% for all assays at low and intermediate thresholds. Specificity increased with higher thresholds and was above 90% for all assays with intermediate and high thresholds. Specificity of AcuStar HIT-IgG (92.8%; 95% CI 87.7, 96.2) was significantly higher than PaGIA (83.0%; 95% CI 76.3, 88.5) and higher than ELISA (81.8%, 95% CI 74.2, 88.0) at low threshold (p<0.05). Reproducibility was adequate for all assays. Total costs per test were CHF 51.02 for ELISA, 117.70 for AcuStar HIT-IgG, and 83.13 for PaGIA.
We observed favourable diagnostic accuracy measures and a high reproducibility for PaGIA and AcuStar HIT-IgG. Implementation into 24-hours-service might improve patient care but the results must be confirmed in other settings and larger populations as well.
免疫测定在疑似肝素诱导的血小板减少症(HIT)患者的检查中至关重要,并且最近已经开发出快速检测方法。然而,关于不同免疫测定在临床实践中的诊断准确性、可重复性和分析成本的比较数据有限。
对179例在临床实践中使用多特异性酶联免疫吸附测定(GTI诊断公司;ELISA)和快速颗粒凝胶免疫测定(PaGIA)评估疑似HIT的连续患者样本,另外用IgG特异性化学发光免疫测定(AcuStar HIT-IgG)进行分析。HIT的存在定义为功能性肝素诱导血小板聚集试验呈阳性。按照先前确定的低、中、高阈值(ELISA:光密度分别为0.4、1.3和2.0;PaGIA:阳性/阴性、滴度为4、滴度为32;AcuStar HIT-IgG:1.0 U/ml、2.8、9.4)确定诊断准确性,并通过重复测量评估可重复性。根据瑞士医疗保健系统,考虑试剂、对照和技术人员的工作时间来计算检测成本。
171例患者(95.5%)有PaGIA结果数据,144例患者(80.4%)有ELISA结果数据,179例患者(100%)有AcuStar HIT-IgG结果数据。在低阈值和中阈值时,所有检测方法的敏感性均高于95%。特异性随阈值升高而增加,在中阈值和高阈值时,所有检测方法的特异性均高于90%。在低阈值时,AcuStar HIT-IgG的特异性(92.8%;95%可信区间87.7, 96.2)显著高于PaGIA(83.0%;95%可信区间76.3, 88.5),且高于ELISA(81.8%,95%可信区间74.2, 88.0)(p<0.05)。所有检测方法的可重复性都足够。ELISA每次检测的总成本为51.02瑞士法郎,AcuStar HIT-IgG为117.70瑞士法郎,PaGIA为83.13瑞士法郎。
我们观察到PaGIA和AcuStar HIT-IgG具有良好的诊断准确性指标和高可重复性。实施24小时服务可能会改善患者护理,但结果必须在其他环境和更大人群中得到证实。