Calcaianu George, Calcaianu Mihaela, Canuet Matthieu, Enache Irina, Kessler Romain
1 Service de Pneumologie, Fédération de médecine translationnelle de Strasbourg, Nouvel Hôpital Civil, Université de Strasbourg, Strasbourg, France.
2 Service de Cardiologie, Nouvel Hôpital Civil, Université de Strasbourg, France.
Pulm Circ. 2017 Apr-Jun;7(2):439-447. doi: 10.1177/2045893217702401. Epub 2017 Mar 13.
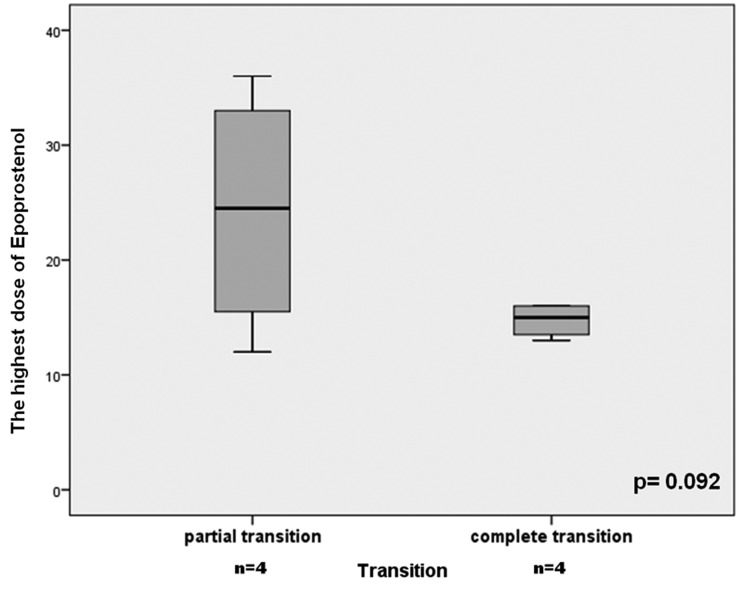
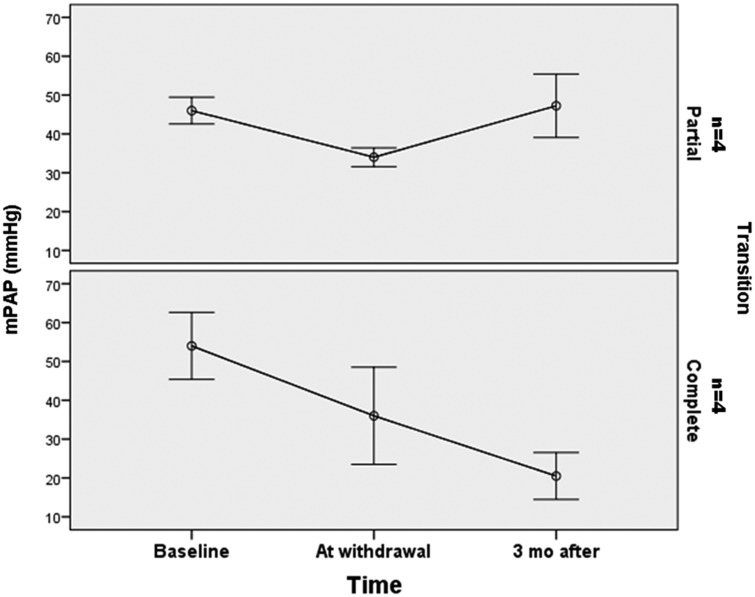
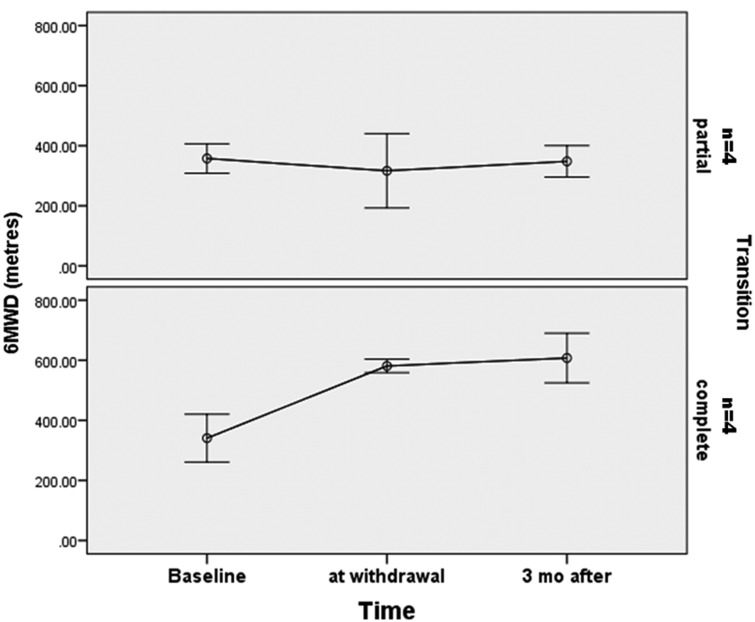
Once initiated for pulmonary arterial hypertension (PAH), epoprostenol treatment usually needs to be delivered for an indefinite duration. It is possible that some participants could be transitioned from epoprostenol to oral therapies. We retrospectively evaluated eight PAH participants transitioned from epoprostenol to PAH oral drugs. The criteria for epoprostenol withdrawal were: (1) persistent improvement of clinic and hemodynamic status; (2) stable dose of epoprostenol for the last three months; and (3) the participant's preference for oral therapy after evaluation of risk-benefit. We evaluated the clinical, functional, and hemodynamic status at baseline, at withdrawal, and after the transition to oral PAH therapy. The transition was completed in all eight participants. Four participants had a complete successful transition (CT) with a stable clinical and hemodynamic course and four participants had a partial successful transition (PT) remaining stable clinically, with a mild hemodynamic worsening, but without need to re-initiate epoprostenol therapy. The four CT participants were treated with epoprostenol for a shorter period of time (CT group: 35 ± 30 versus PT group: 79 ± 49 months, P = 0.08). Mean epoprostenol dosage was lower in the CT group (CT group: 15 ± 1.5 ng/kg/min versus PT group: 24 ± 11 ng/kg/min, P = 0.09). Safe withdrawal of epoprostenol treatment and transition to oral PAH therapy was possible in a small and highly selected group of participants. The majority of these participants had a porto-pulmonary PAH or PAH associated to HIV infection.
一旦开始用于治疗肺动脉高压(PAH),依前列醇治疗通常需要持续不定的时间。部分参与者有可能从依前列醇转换为口服疗法。我们回顾性评估了8名从依前列醇转换为PAH口服药物的参与者。依前列醇撤药标准为:(1)临床和血流动力学状态持续改善;(2)过去三个月依前列醇剂量稳定;(3)参与者在评估风险效益后倾向于口服治疗。我们评估了基线、撤药时以及转换为PAH口服治疗后的临床、功能和血流动力学状态。所有8名参与者均完成了转换。4名参与者实现了完全成功转换(CT),临床和血流动力学过程稳定,4名参与者实现了部分成功转换(PT),临床保持稳定,血流动力学有轻度恶化,但无需重新开始依前列醇治疗。4名CT参与者接受依前列醇治疗的时间较短(CT组:35±30个月,PT组:79±49个月,P = 0.08)。CT组的依前列醇平均剂量较低(CT组:15±1.5 ng/kg/min,PT组:24±11 ng/kg/min,P = 0.09)。在一小部分经过严格挑选的参与者中,依前列醇治疗的安全撤药以及向PAH口服治疗的转换是可行的。这些参与者大多数患有门静脉-肺动脉高压或与HIV感染相关的PAH。