Samaraweera Sahan Asela, Gibbons Berwyck, Gour Anami, Sedgwick Philip
Medical School, St. George's University of London, London, UK.
Paediatric Intensive Care Unit (PICU), St. George's University Hospitals NHS Foundation Trust, London, SW17 0QT, UK.
Eur J Pediatr. 2017 Aug;176(8):1055-1060. doi: 10.1007/s00431-017-2925-9. Epub 2017 Jun 10.
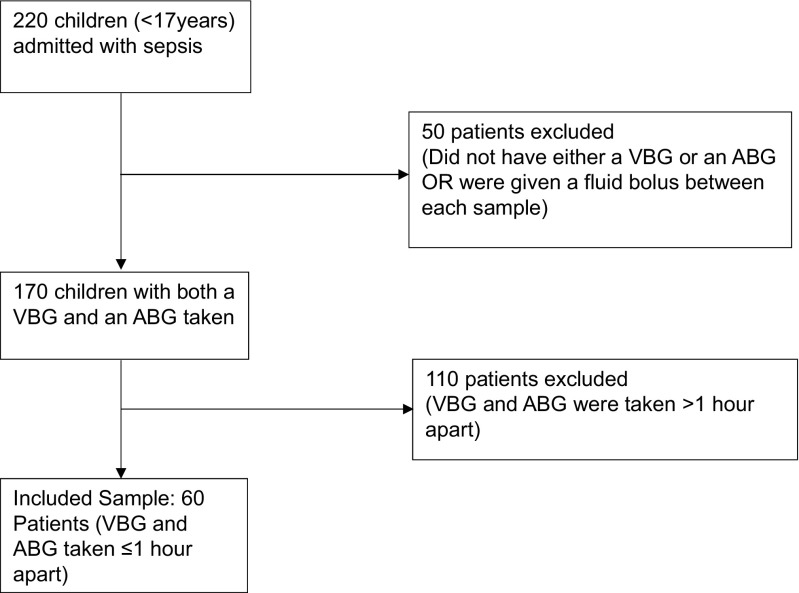
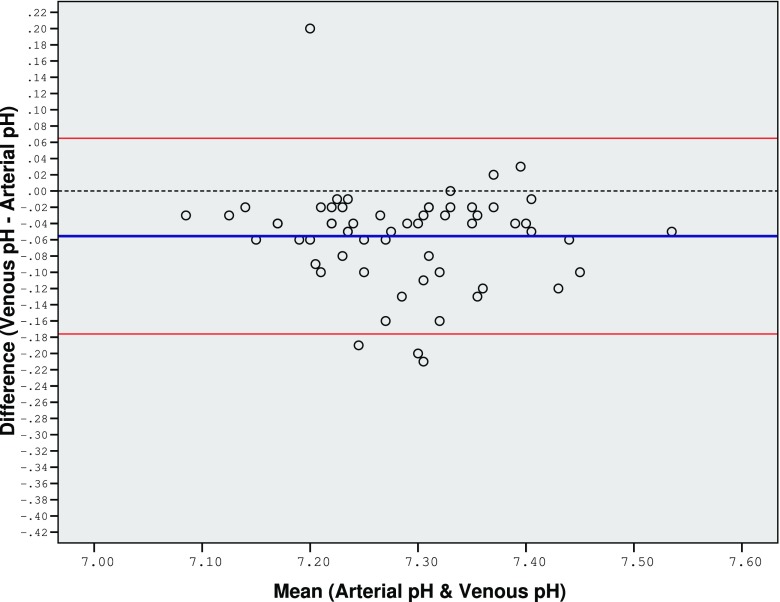
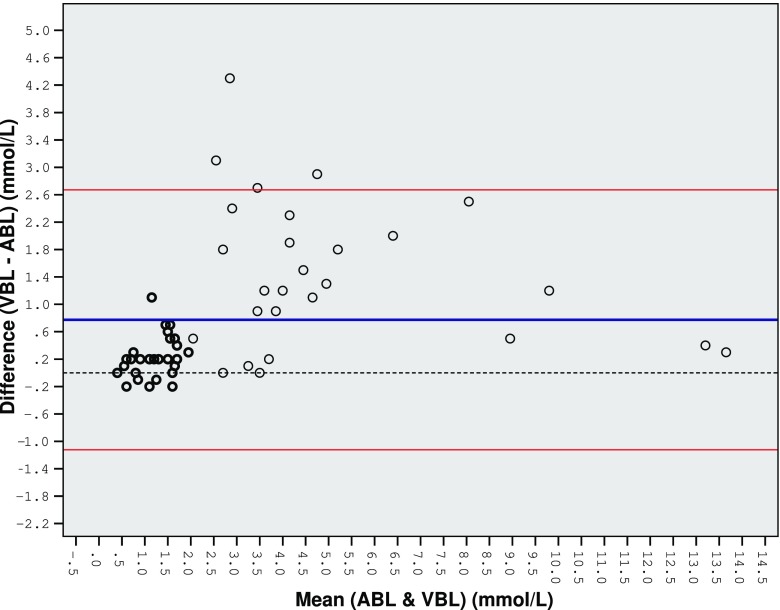
This study assessed the agreement between arterial and venous blood lactate and pH levels in children with sepsis. This retrospective, three-year study involved 60 PICU patients, with data collected from electronic or paper patient records. The inclusion criteria comprised of children (≤17 years old) with sepsis and those who had a venous blood gas taken first with an arterial blood gas taken after within one hour. The lactate and pH values measured through each method were analysed. There is close agreement between venous and arterial lactate up to 2 mmol/L. As this value increases, this agreement becomes poor. The limits of agreement (LOA) are too large (±1.90 mmol/L) to allow venous and arterial lactate to be used interchangeably. The mean difference and LOA between both methods would be much smaller if derived using lactate values under 2.0 mmol/L. There is close agreement between arterial and venous pH (MD = -0.056, LOA ± 0.121). However, due to extreme variations in pH readings during sepsis, pH alone is an inadequate marker.
A venous lactate ≤2 mmol/L can be used as a surrogate for arterial lactate during early management of sepsis in children. However, if the value exceeds 2 mmol/L, an arterial sample must confirm the venous result. What is known: • In children with septic shock, a blood gas is an important test to show the presence of acidosis and high lactic acid. Hyperlactataemia on admission is an early predictor of outcome and is associated with a greater mortality risk. • An arterial sample is the standard for lactate measurement, however getting a sample may be challenging in the emergency department or a general paediatric ward. Venous samples are quicker and easier to obtain. Adult studies generally advise caution in replacing venous lactate values for the arterial standard, whilst paediatric studies are limited in this area. What is new: • This is the first study assessing the agreement between arterial and peripheral venous lactate in children with sepsis, with a significant sample of patients. • This study shows that a venous sample with a lactate of ≤ 2 mmol/L can be used as a surrogate measurement for arterial lactate during early management of sepsis in children. However, if the venous lactate is above 2 mmol/L, an arterial sample must be taken to confirm the result.
本研究评估了脓毒症患儿动脉血与静脉血乳酸及pH值之间的一致性。这项为期三年的回顾性研究纳入了60名儿科重症监护病房(PICU)患者,数据从电子或纸质病历中收集。纳入标准包括患有脓毒症的儿童(≤17岁)以及那些先采集静脉血气样本,随后在1小时内采集动脉血气样本的患儿。对通过每种方法测得的乳酸和pH值进行了分析。静脉血与动脉血乳酸在2 mmol/L以内时一致性良好。随着该值升高,这种一致性变差。一致性界限(LOA)过大(±1.90 mmol/L),以至于不能将静脉血和动脉血乳酸互换使用。如果使用2.0 mmol/L以下的乳酸值得出两种方法之间的平均差异和LOA会小得多。动脉血与静脉血pH之间一致性良好(平均差 = -0.056,LOA ± 0.121)。然而,由于脓毒症期间pH读数变化极大,仅pH值作为指标并不充分。
在儿童脓毒症早期管理中,静脉血乳酸≤2 mmol/L可作为动脉血乳酸的替代指标。然而,如果该值超过2 mmol/L,必须采集动脉血样本以确认静脉血检测结果。已知信息:• 在感染性休克患儿中,血气分析是显示酸中毒和高乳酸血症存在的重要检查。入院时高乳酸血症是预后的早期预测指标,且与更高的死亡风险相关。• 动脉血样本是乳酸测量的标准,但在急诊科或普通儿科病房获取样本可能具有挑战性。静脉血样本采集更快且更容易。成人研究一般建议谨慎使用静脉血乳酸值替代动脉血标准,而儿科在这方面的研究有限。新发现:• 这是第一项对大量脓毒症患儿动脉血与外周静脉血乳酸一致性进行评估的研究。• 本研究表明,在儿童脓毒症早期管理中,乳酸≤2 mmol/L的静脉血样本可作为动脉血乳酸的替代测量指标。然而,如果静脉血乳酸高于2 mmol/L,必须采集动脉血样本以确认结果。