Imada Hiroshi, Fukuzawa Koji, Kiuchi Kunihiko, Matsumoto Akinori, Konishi Hiroki, Ichibori Hirotoshi, Hyogo Kiyohiro, Kurose Jun, Mori Shumpei, Takaya Tomofumi, Nishii Tatsuya, Kagawa Kiyosumi, Yoshida Akihiro, Ken-Ichi Hirata
Section of Arrhythmia, Division of Cardiovascular Medicine, Department of Internal Medicine, Kobe University Graduate School of Medicine, Japan.
Division of Cardiovascular Medicine, Department of Internal Medicine, Kobe University Graduate School of Medicine, Japan.
J Arrhythm. 2017 Jun;33(3):177-184. doi: 10.1016/j.joa.2016.10.003. Epub 2016 Oct 27.
The relationship between pulmonary vein (PV) arrhythmogenicity and its anatomy has been reported. However, that of the superior vena cava (SVC) has not been well discussed. Arrhythmogenic response induced by pacing stimulation at SVC might help with identifying SVC arrhythmogenicity. The purpose of this study was to investigate the relationship between the anatomical dilatation of SVC and the arrhythmogenic response induced by pacing at SVC.
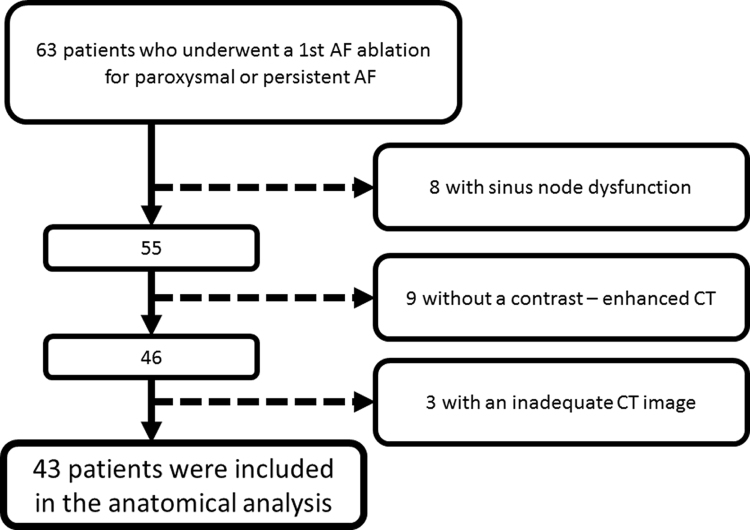
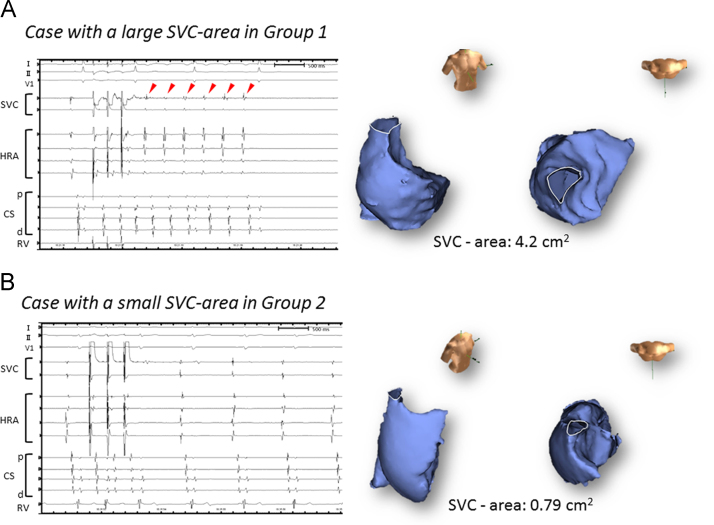
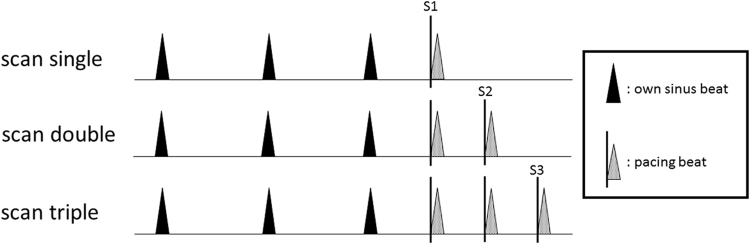
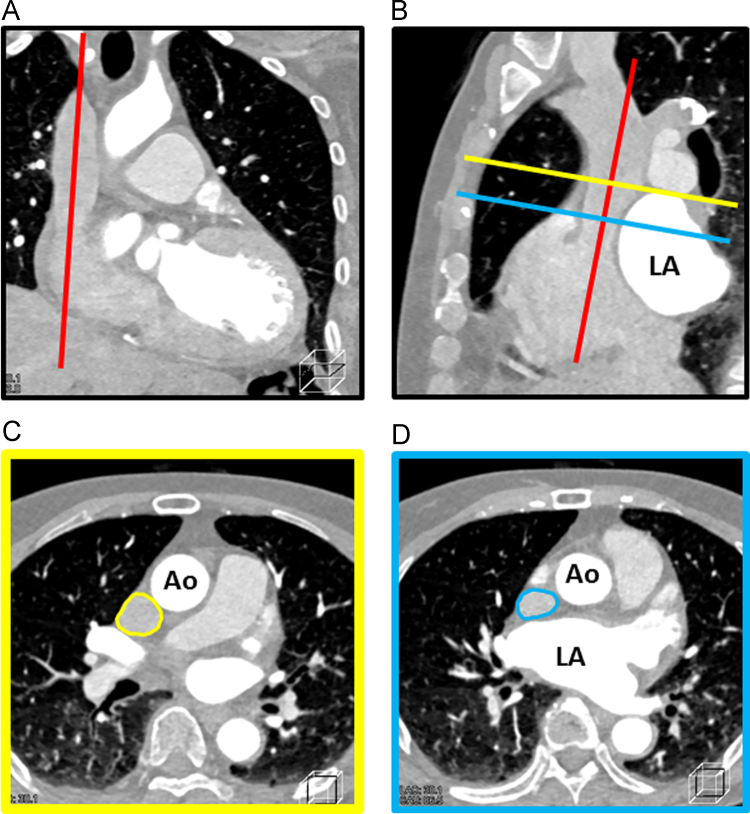
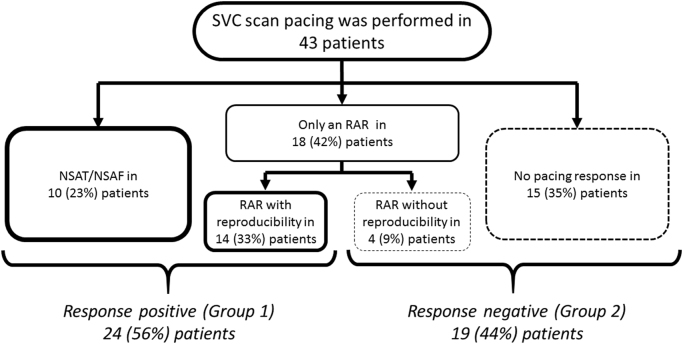
Forty-three patients who underwent atrial fibrillation (AF) ablation were enrolled in this study. After PV isolation, scan pacing (up to triple extra stimulation following intrinsic sinus beats) was performed at SVC. The arrhythmogenic response was defined as following: (1) repetitive atrial responses, (2) non-sustained, and (3) sustained AF/ atrial tachycardia. To assess the dilatation of SVC, we measured the cross-sectional area of the SVC (SVC-area) using multi-planar reconstruction CT imaging.
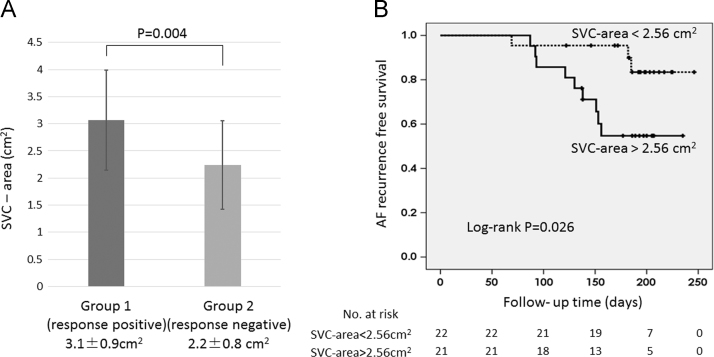
Arrhythmogenic responses were documented in 24 patients (Group 1). No arrhythmogenic responses were documented in the remaining 19 patients (Group 2). The SVC-area was significantly larger in Group 1 than Group 2 (3.1±0.9 vs. 2.2±0.8 cm, =0.004). A multivariate analysis revealed only SVC-area was associated with arrhythmogenic responses (odds ratio=2.87, CI 1.05-7.82, =0.04). Furthermore, AF recurrence rate was significantly higher in patients with SVC-area>2.56 cm than those with SVC-area <2.56 cm (9 [42.9%] of 21 vs. 3 [13.6%] of 22, =0.026).
Dilatation of SVC was associated with an arrhythmogenic response, and the AF recurrence rate was significantly higher in patients with large SVC-area. Adjunctive catheter intervention for the SVC might be indicated in patients with a dilated SVC and an arrhythmogenic response.
肺静脉(PV)致心律失常性与其解剖结构之间的关系已有报道。然而,上腔静脉(SVC)的相关关系尚未得到充分讨论。在SVC进行起搏刺激所诱发的致心律失常反应可能有助于识别SVC的致心律失常性。本研究的目的是探讨SVC的解剖扩张与SVC起搏诱发的致心律失常反应之间的关系。
43例行房颤(AF)消融术的患者纳入本研究。在肺静脉隔离后,于SVC进行扫描起搏(在固有窦性搏动后最多进行三次额外刺激)。致心律失常反应定义如下:(1)重复性心房反应,(2)非持续性,以及(3)持续性房颤/房性心动过速。为评估SVC的扩张情况,我们使用多平面重建CT成像测量SVC的横截面积(SVC面积)。
24例患者(第1组)记录到致心律失常反应。其余19例患者(第2组)未记录到致心律失常反应。第1组的SVC面积显著大于第2组(3.1±0.9 vs. 2.2±0.8 cm²,P = 0.004)。多因素分析显示只有SVC面积与致心律失常反应相关(比值比 = 2.87,CI 1.05 - 7.82,P = 0.04)。此外,SVC面积>2.56 cm²的患者房颤复发率显著高于SVC面积<2.56 cm²的患者(21例中的9例[42.9%] vs. 22例中的3例[13.6%],P = 0.026)。
SVC扩张与致心律失常反应相关,SVC面积大的患者房颤复发率显著更高。对于SVC扩张且有致心律失常反应的患者,可能需要对SVC进行辅助导管干预。