Yabuuchi Junko, Suwabe Tatsuya, Mizuno Hiroki, Ueno Toshiharu, Hoshino Junichi, Sekine Akinari, Kawada Masahiro, Yamanouchi Masayuki, Hayami Noriko, Hiramatsu Rikako, Hasegawa Eiko, Sawa Naoki, Takaichi Kenmei, Fujii Takeshi, Ohashi Kenichi, Ubara Yoshifumi
Nephrology Center, Toranomon Hospital, Japan.
Okinaka Memorial Institute for Medical Research, Toranomon Hospital, Japan.
Intern Med. 2017;56(12):1543-1547. doi: 10.2169/internalmedicine.56.8081. Epub 2017 Jun 15.
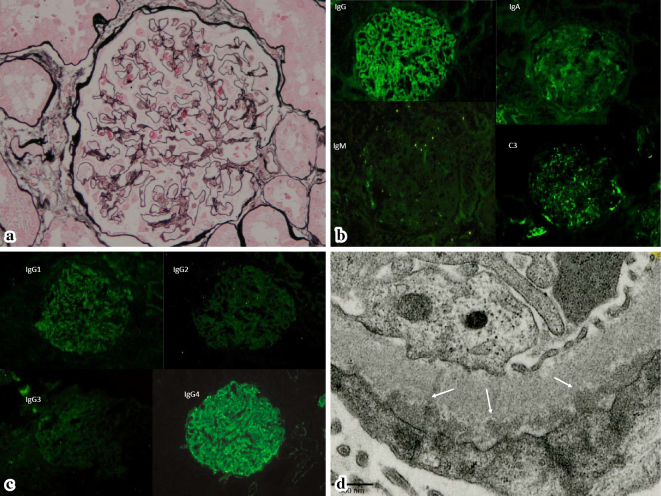
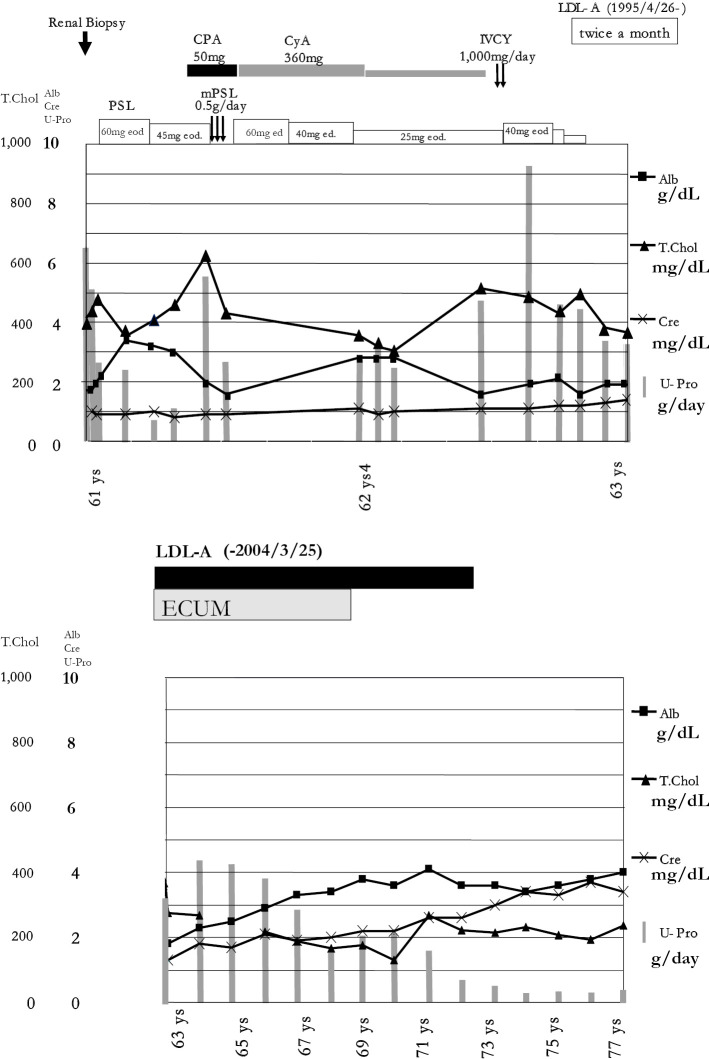
A 61-year-old Japanese man developed nephrotic syndrome (NS) due to idiopathic membranous glomerulonephritis (MGN). He received immunosuppressive therapy for two years, including prednisolone, cyclophosphamide, and cyclosporine A, but the NS persisted. Low-density lipoprotein apheresis (LDL-A) was initiated at a frequency of twice a month and continued for 9 years (203 sessions in total). His proteinuria reduced to less than 1 g daily after 9 years. LDL-A was stopped, and the NS has not relapsed for five years. This case suggests that long-term LDL-A therapy may be a treatment option for idiopathic MGN refractory to immunosuppressive therapy or short-term LDL-A.
一名61岁的日本男性因特发性膜性肾小球肾炎(MGN)发展为肾病综合征(NS)。他接受了两年的免疫抑制治疗,包括泼尼松龙、环磷酰胺和环孢素A,但肾病综合征仍持续存在。开始每月进行两次低密度脂蛋白去除术(LDL-A),并持续了9年(共203次)。9年后,他的蛋白尿减少到每日少于1克。停止了LDL-A治疗,肾病综合征已五年未复发。该病例表明,长期LDL-A治疗可能是免疫抑制治疗或短期LDL-A治疗无效的特发性MGN的一种治疗选择。