Katikireddi Srinivasa Vittal, Whitley Elise, Lewsey Jim, Gray Linsay, Leyland Alastair H
Medical Research Council (MRC)/Scottish Government Chief Scientist Office (CSO) Social and Public Health Sciences Unit, University of Glasgow, Glasgow, UK.
Medical Research Council (MRC)/Scottish Government Chief Scientist Office (CSO) Social and Public Health Sciences Unit, University of Glasgow, Glasgow, UK.
Lancet Public Health. 2017 May 10;2(6):e267-e276. doi: 10.1016/S2468-2667(17)30078-6. eCollection 2017 Jun.
Alcohol-related mortality and morbidity are high in socioeconomically disadvantaged populations compared with individuals from advantaged areas. It is unclear if this increased harm reflects differences in alcohol consumption between these socioeconomic groups, reverse causation (ie, downward social selection for high-risk drinkers), or a greater risk of harm in individuals of low socioeconomic status compared with those of higher status after similar consumption. We aimed to investigate whether the harmful effects of alcohol differ by socioeconomic status, accounting for alcohol consumption and other health-related factors.
The Scottish Health Surveys are record-linked cross-sectional surveys representative of the adult population of Scotland. We obtained baseline demographics and data for alcohol consumption (units per week and binge drinking) from Scottish Health Surveys done in 1995, 1998, 2003, 2008, 2009, 2010, 2011, and 2012. We matched these data to records for deaths, admissions, and prescriptions. The primary outcome was alcohol-attributable admission or death. The relation between alcohol-attributable harm and socioeconomic status was investigated for four measures (education level, social class, household income, and area-based deprivation) using Cox proportional hazards models. The potential for alcohol consumption and other risk factors (including smoking and body-mass index [BMI]) mediating social patterning was explored in separate regression models. Reverse causation was tested by comparing change in area deprivation over time.
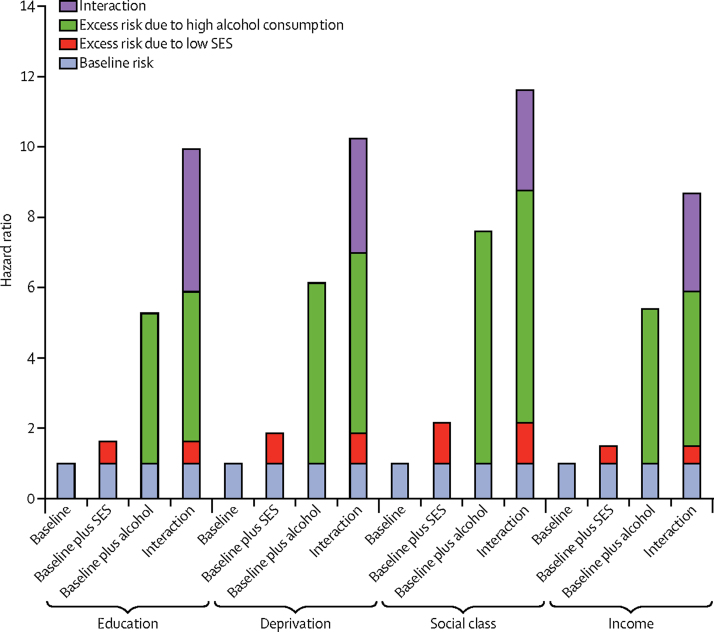
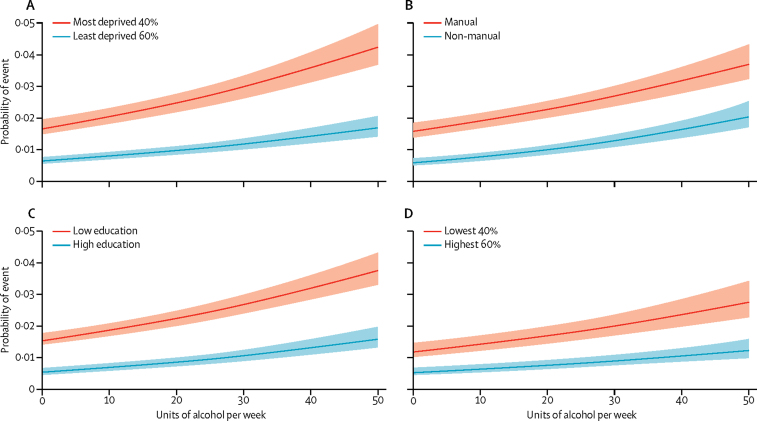
50 236 participants (21 777 men and 28 459 women) were included in the analytical sample, with 429 986 person-years of follow-up. Low socioeconomic status was associated consistently with strikingly raised alcohol-attributable harms, including after adjustment for weekly consumption, binge drinking, BMI, and smoking. Evidence was noted of effect modification; for example, relative to light drinkers living in advantaged areas, the risk of alcohol-attributable admission or death for excessive drinkers was increased (hazard ratio 6·12, 95% CI 4·45-8·41 in advantaged areas; and 10·22, 7·73-13·53 in deprived areas). We found little support for reverse causation.
Disadvantaged social groups have greater alcohol-attributable harms compared with individuals from advantaged areas for given levels of alcohol consumption, even after accounting for different drinking patterns, obesity, and smoking status at the individual level.
Medical Research Council, NHS Research Scotland, Scottish Government Chief Scientist Office.
与来自富裕地区的个体相比,社会经济地位不利人群中与酒精相关的死亡率和发病率较高。目前尚不清楚这种危害增加是否反映了这些社会经济群体之间饮酒量的差异、反向因果关系(即高风险饮酒者的社会地位下降),或者在饮酒量相似的情况下,社会经济地位较低的个体与较高地位的个体相比,危害风险更大。我们旨在调查酒精的有害影响是否因社会经济地位而异,并考虑饮酒量和其他与健康相关的因素。
苏格兰健康调查是与记录相链接的横断面调查,代表了苏格兰成年人口。我们从1995年、1998年、2003年、2008年、2009年、2010年、2011年和2012年进行的苏格兰健康调查中获取了基线人口统计学数据和饮酒量(每周单位数和暴饮)数据。我们将这些数据与死亡、住院和处方记录进行匹配。主要结局是酒精导致的住院或死亡。使用Cox比例风险模型,针对四项指标(教育水平、社会阶层、家庭收入和地区贫困程度)调查了酒精导致的危害与社会经济地位之间的关系。在单独的回归模型中探讨了饮酒量和其他风险因素(包括吸烟和体重指数[BMI])介导社会模式的可能性。通过比较不同时间地区贫困程度的变化来检验反向因果关系。
分析样本包括50236名参与者(21777名男性和28459名女性),随访时间为429986人年。社会经济地位低始终与酒精导致的危害显著增加相关,包括在调整每周饮酒量、暴饮、BMI和吸烟后。注意到有效应修正的证据;例如,相对于生活在富裕地区的轻度饮酒者,过度饮酒者酒精导致的住院或死亡风险增加(富裕地区风险比6.12,95%CI 4.45 - 8.41;贫困地区为10.22,7.73 - 13.53)。我们几乎没有找到反向因果关系的证据。
对于给定的饮酒量水平,即使在考虑了个体层面不同的饮酒模式、肥胖和吸烟状况之后,社会经济地位不利群体与来自富裕地区的个体相比,酒精导致的危害更大。
医学研究理事会、苏格兰国民保健服务研究、苏格兰政府首席科学家办公室。