Chen Haifei, Fu Ailin, Wang Jing, Wu Tianqin, Li Zhengyang, Tang Jieqing, Shen Hongshi, Zhu Jingjing, Li Jie, Zhu Qian, Qing Longmei
1 Department of Hematology, 100th hospital of People's Liberation Army, Suzhou City, Jiangsu Province, China.
2 Division of Hematology and Oncology, The First People's Hospital of Kunshan, Jiangsu Province, China.
J Int Med Res. 2017 Jun;45(3):1253-1260. doi: 10.1177/0300060517695646. Epub 2017 Mar 21.
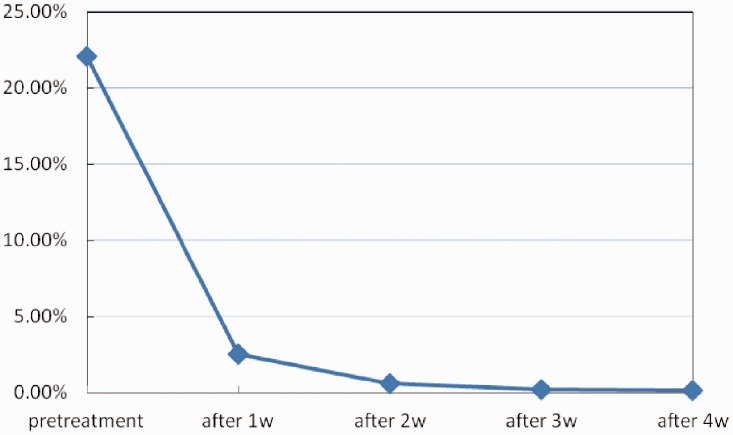
Objective To investigate the efficacy and safety of rituximab (RTX) as first-line treatment of acquired thrombotic thrombocytopenic purpura (aTTP). Methods Twenty-five patients with acute aTTP and/or severe a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 (ADAMTS13) deficiency were admitted to our centre from April 2009 to March 2015. Fourteen patients received RTX plus standard therapy (plasma exchange and corticosteroids) at acute episodes. Haemoglobin, platelet count, schistocytes, lactate dehydrogenase levels, ADAMTS13 activity and its inhibitors, and the ratio of B lymphocytes in the peripheral blood, were monitored. The number of plasma exchange (PEXs), total plasma volume, remission time, relapse ratio, and adverse effects were recorded. Results The median number of PEXs was 5 (2-17) sessions and median total plasma volume was 168.43 ml/kg (62.86-469.52 ml/kg). Patients achieved haematological remission at a median of 15 days (5-22 days), and the median time of immunological remission was 2 weeks (2-8 weeks) with a median follow-up of 13 months (3-61 months). ADAMTS13 activity significantly increased after 2 weeks. The B lymphocyte percentage in peripheral blood was reduced 1 week after the first dose of RTX infusion compared with before treatment (2.21% ± 5.23% vs 18.47% ± 7.34%, P = 0.000 [the result of statistical software]), and began to gradually increase 9 months later. Severe adverse effects and relapsing TTP were not observed during therapy and follow-up. However, one patient who had sustained immunological remission died of severe pneumonia 7 months later. Conclusion Although our study was limited by its small sample number and it was a non-controlled, clinical trial, it showed potential benefits of RTX therapy for acute aTTP. RTX may be administered as a first-line therapy for lowering patients' relapse rate in the long term. Randomized, controlled trials of RTX for aTTP are required.
目的 探讨利妥昔单抗(RTX)作为获得性血栓性血小板减少性紫癜(aTTP)一线治疗的疗效和安全性。方法 2009年4月至2015年3月,25例急性aTTP和/或严重的含Ⅰ型血小板反应蛋白基序的解聚素和金属蛋白酶13(ADAMTS13)缺乏患者入住本中心。14例患者在急性发作期接受RTX加标准治疗(血浆置换和皮质类固醇)。监测血红蛋白、血小板计数、裂体细胞、乳酸脱氢酶水平、ADAMTS13活性及其抑制剂,以及外周血B淋巴细胞比例。记录血浆置换(PEXs)次数、总血浆量、缓解时间、复发率及不良反应。结果 PEXs中位数为5(2~17)次,总血浆量中位数为168.43 ml/kg(62.86~469.52 ml/kg)。患者血液学缓解的中位时间为15天(5~22天),免疫缓解的中位时间为2周(2~8周),中位随访时间为13个月(3~61个月)。2周后ADAMTS13活性显著增加。与治疗前相比,首次输注RTX 1周后外周血B淋巴细胞百分比降低(2.21%±5.23%对18.47%±7.34%,P = 0.000[统计软件结果]),9个月后开始逐渐升高。治疗及随访期间未观察到严重不良反应和复发性TTP。然而,1例持续免疫缓解的患者7个月后死于重症肺炎。结论 尽管本研究受样本量小且为非对照临床试验的限制,但显示RTX治疗急性aTTP有潜在益处。RTX可作为一线治疗以长期降低患者复发率。需要对RTX治疗aTTP进行随机对照试验。