Caspi Oren, Habib Manhal, Cohen Yuval, Kerner Arthur, Roguin Ariel, Abergel Eitan, Boulos Monther, Kapeliovich Michael R, Beyar Rafael, Nikolsky Eugenia, Aronson Doron
Department of Cardiology, Rambam Medical Center, Haifa, Israel.
B. Rappaport Faculty of Medicine, Technion Medical School, Haifa, Israel.
J Am Heart Assoc. 2017 Jun 24;6(6):e005715. doi: 10.1161/JAHA.117.005715.
Acute kidney injury (AKI) following primary percutaneous coronary intervention (pPCI) is frequently interpreted as contrast-induced AKI but may result from other insults. We aimed to determine the causal association of contrast material exposure and the incidence of AKI following pPCI using a control group of propensity score-matched patients with ST-segment-elevation myocardial infarction who were not exposed to contrast material.
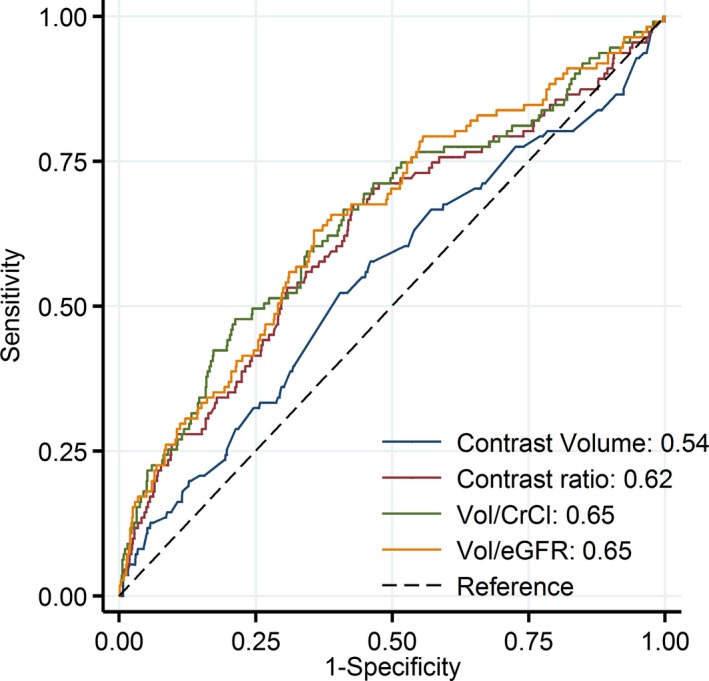
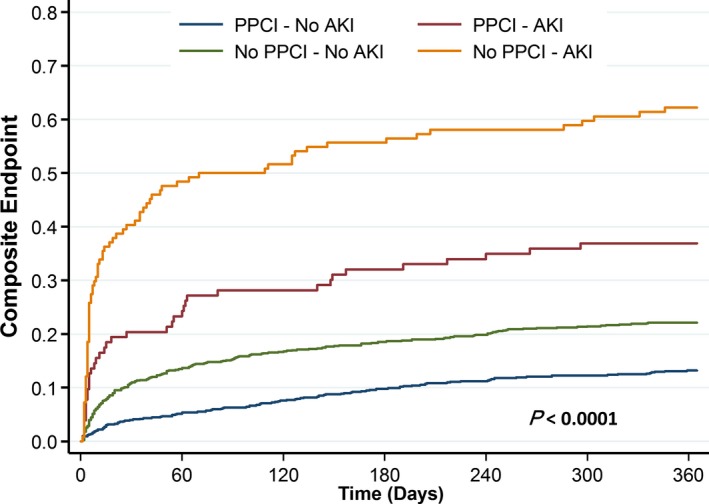
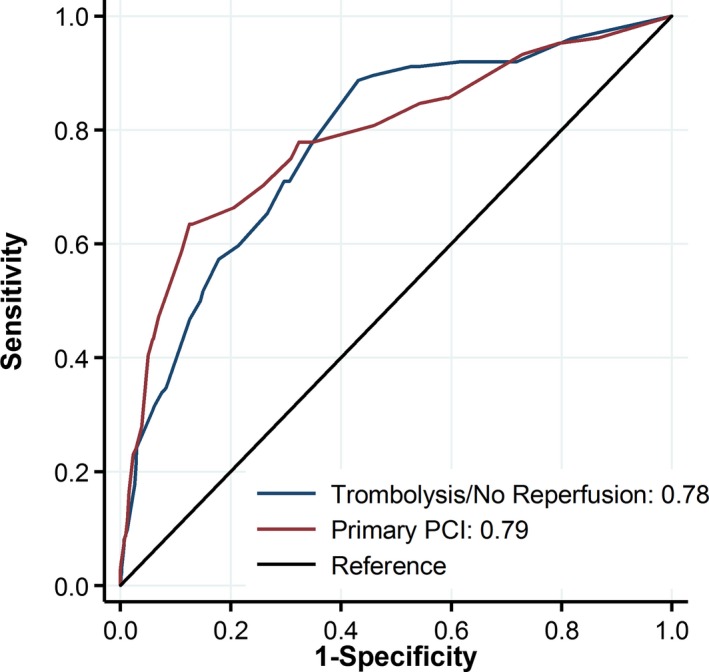
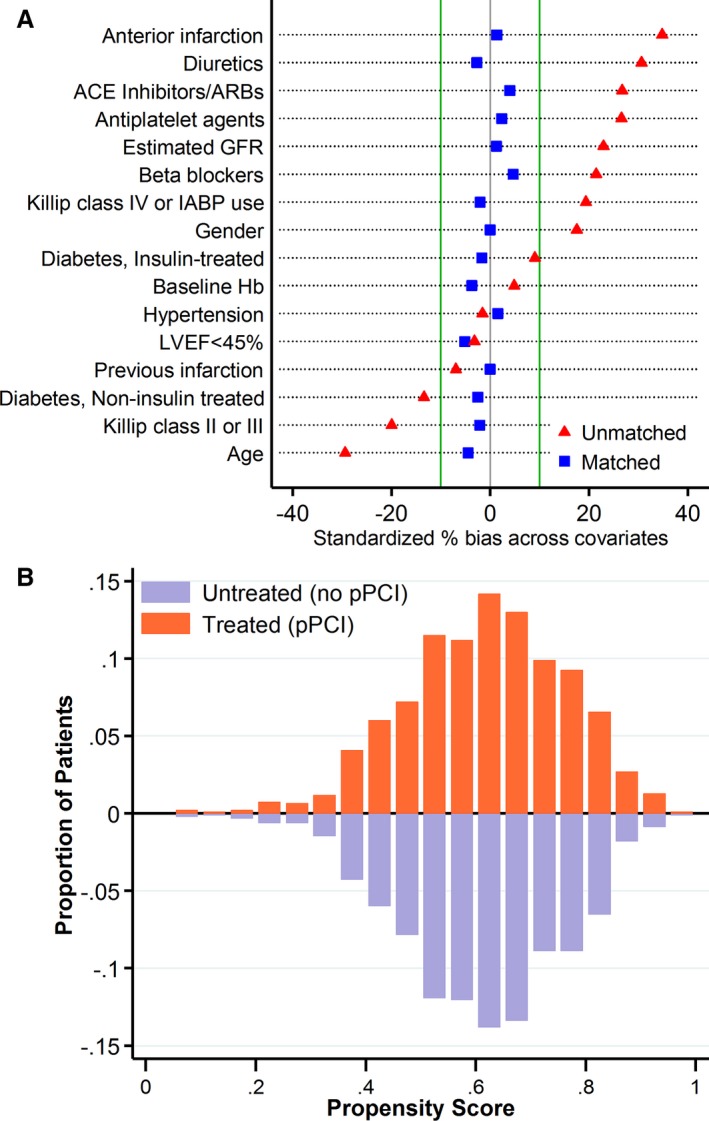
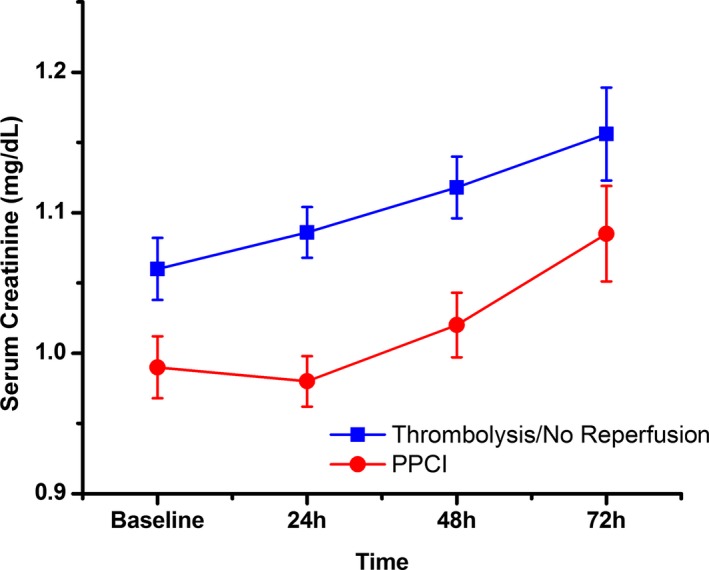
We studied 2025 patients with ST-segment-elevation myocardial infarction who underwent pPCI and 1025 patients receiving fibrinolysis or no reperfusion who were not exposed to contrast material during the first 72 hours of hospital stay (control group). AKI was defined as creatinine of ≥0.5 mg/dL or >25% rise within 72 hours. AKI rates were similar in the pPCI and control groups (10.3% versus 12.1%, respectively; =0.38). Propensity score matching resulted in 931 matched pairs with PCI and no PCI, with balanced baseline covariates (standardized difference <0.1). Among propensity score-matched patients, AKI rates were not significantly different with and without PCI (8.6% versus 10.9%, =0.12). In the pPCI cohort, independent predictors of AKI included age ≥70 years, insulin-treated diabetes mellitus, diuretic therapy, anterior infarction, baseline estimated glomerular filtration rate, and variables related to the presence of pump failure (higher Killip class, intra-aortic balloon pump use) and reduced left ventricular ejection fraction but not contrast material dose. A risk score based on the PCI cohort had similar discriminatory capacity for AKI in the control group (C statistic 0.81±0.02 and 0.78±0.02, respectively; =0.26).
The development of AKI in patients with ST-segment-elevation myocardial infarction undergoing pPCI is mainly related to older age, baseline estimated glomerular filtration rate, heart failure, and hemodynamic instability. Risk for AKI is similar among ST-segment-elevation myocardial infarction patients with and without contrast material exposure.
直接经皮冠状动脉介入治疗(pPCI)后发生的急性肾损伤(AKI)常被认为是造影剂所致,但也可能由其他损伤因素引起。我们旨在通过一组倾向评分匹配的未接触造影剂的ST段抬高型心肌梗死患者作为对照组,确定造影剂暴露与pPCI后AKI发生率之间的因果关系。
我们研究了2025例接受pPCI的ST段抬高型心肌梗死患者以及1025例接受溶栓治疗或未进行再灌注治疗且在住院的前72小时内未接触造影剂的患者(对照组)。AKI定义为肌酐水平≥0.5mg/dL或在72小时内升高>25%。pPCI组和对照组的AKI发生率相似(分别为10.3%和12.1%;P=0.38)。倾向评分匹配产生了931对匹配的接受PCI和未接受PCI的患者,其基线协变量均衡(标准化差异<0.1)。在倾向评分匹配的患者中,接受PCI和未接受PCI的患者的AKI发生率无显著差异(8.6%对10.9%,P=0.12)。在pPCI队列中,AKI的独立预测因素包括年龄≥70岁、胰岛素治疗的糖尿病、利尿剂治疗、前壁心肌梗死、基线估计肾小球滤过率以及与泵衰竭相关的变量(较高的Killip分级、主动脉内球囊反搏使用)和左心室射血分数降低,但不包括造影剂剂量。基于pPCI队列的风险评分在对照组中对AKI具有相似的鉴别能力(C统计量分别为0.81±0.02和0.78±0.02;P=0.26)。
接受pPCI的ST段抬高型心肌梗死患者发生AKI主要与高龄、基线估计肾小球滤过率、心力衰竭和血流动力学不稳定有关。ST段抬高型心肌梗死患者中,接触造影剂和未接触造影剂的患者发生AKI的风险相似。