Schiff Gordon D, Reyes Nieva Harry, Griswold Paula, Leydon Nicholas, Ling Judy, Federico Frank, Keohane Carol, Ellis Bonnie R, Foskett Cathy, Orav E John, Yoon Catherine, Goldmann Don, Weissman Joel S, Bates David W, Biondolillo Madeleine, Singer Sara J
*Division of General Internal Medicine and Primary Care, Brigham and Women's Hospital †Harvard Medical School, Boston, MA ‡Johns Hopkins Bloomberg School of Public Health, Baltimore, MD §Massachusetts Coalition for the Prevention of Medical Errors, Burlington ∥Bureau of Health Care Safety and Quality, Massachusetts Department of Public Health, Boston, MA ¶North Shore Medical Center, Salem #Institute for Healthcare Improvement, Cambridge **Risk Management Foundation of the Harvard Medical Institutions (CRICO) ††Coverys Corporation; One Financial Center ‡‡Harvard T.H. Chan School of Public Health §§Center for Surgery and Public Health, Brigham and Women's Hospital ∥∥Mongan Institute for Health Policy, Massachusetts General Hospital, Boston, MA.
Med Care. 2017 Aug;55(8):797-805. doi: 10.1097/MLR.0000000000000759.
Evaluate application of quality improvement approaches to key ambulatory malpractice risk and safety areas.
In total, 25 small-to-medium-sized primary care practices (16 intervention; 9 control) in Massachusetts.
Controlled trial of a 15-month intervention including exposure to a learning network, webinars, face-to-face meetings, and coaching by improvement advisors targeting "3+1" high-risk domains: test result, referral, and medication management plus culture/communication issues evaluated by survey and chart review tools.
Chart reviews conducted at baseline and postintervention for intervention sites. Staff and patient survey data collected at baseline and postintervention for intervention and control sites.
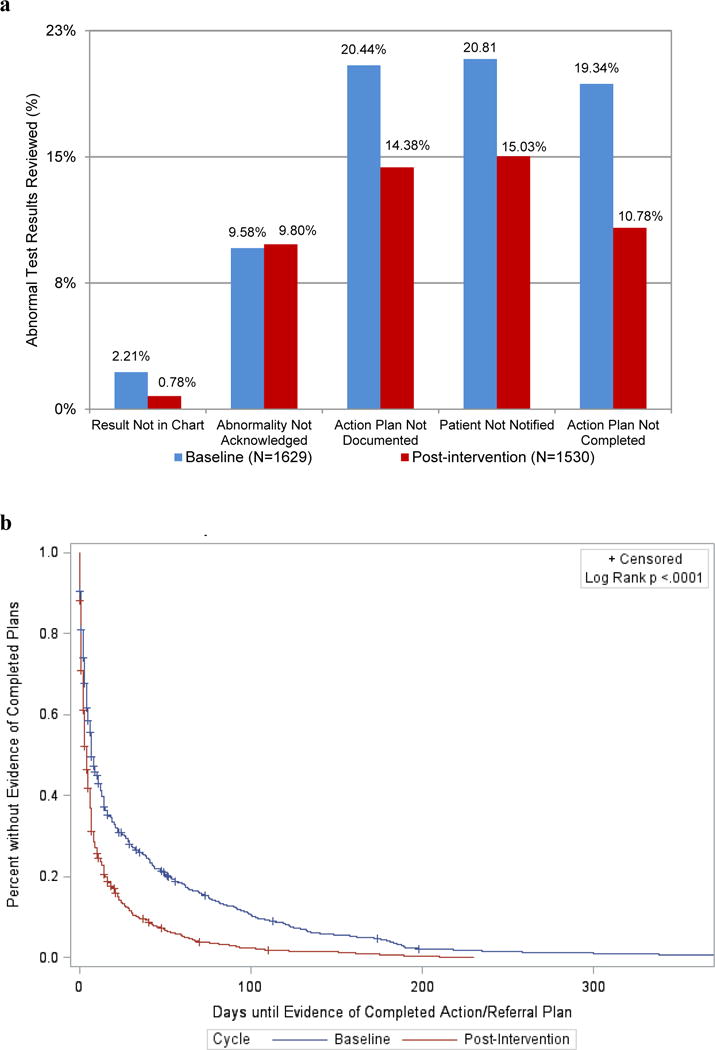
Chart reviews demonstrated significant improvements in documentation of abnormal results, patient notification, documentation of an action or treatment plan, and evidence of a completed plan (all P<0.001). Mean days between laboratory test date and evidence of completed action/treatment plan decreased by 19.4 days (P<0.001). Staff surveys showed modest but nonsignificant improvement for intervention practices relative to controls overall and for the 3 high-risk domains that were the focus of PROMISES.
A consortium of stakeholders, quality improvement tools, coaches, and learning network decreased selected ambulatory safety risks often seen in malpractice claims.
评估质量改进方法在关键门诊医疗过失风险和安全领域的应用。
马萨诸塞州的25家中小型初级医疗诊所(16家干预组;9家对照组)。
一项为期15个月的干预对照试验,包括参与一个学习网络、参加网络研讨会、面对面会议,以及由改进顾问针对“3 + 1”高风险领域进行指导,这几个领域为:检查结果、转诊、药物管理,再加上通过调查和图表审查工具评估的文化/沟通问题。
在干预组站点的基线期和干预后进行图表审查。在干预组和对照组站点的基线期和干预后收集工作人员和患者的调查数据。
图表审查显示,在异常结果记录、患者通知、行动或治疗计划记录以及完整计划的证据方面有显著改善(所有P<0.001)。实验室检查日期与完成行动/治疗计划证据之间的平均天数减少了19.4天(P<0.001)。工作人员调查显示,与对照组总体相比,干预组诊所总体上有适度但不显著的改善,在作为“PROMISES”重点的3个高风险领域也是如此。
由利益相关者、质量改进工具、指导人员和学习网络组成的联盟降低了医疗过失索赔中常见的特定门诊安全风险。