Department of Emergency Medicine, School of Medicine, University of California-Davis, Sacramento, California.
Department of Emergency Medicine, University of Massachusetts Medical School-Baystate, Springfield, Massachusetts.
J Urol. 2017 Dec;198(6):1359-1366. doi: 10.1016/j.juro.2017.06.077. Epub 2017 Jun 23.
More than 1 million patients annually seek care in an emergency department for kidney stones but a minority require hospital admission or a urological procedure. We describe predictors of hospital admission or urological intervention.
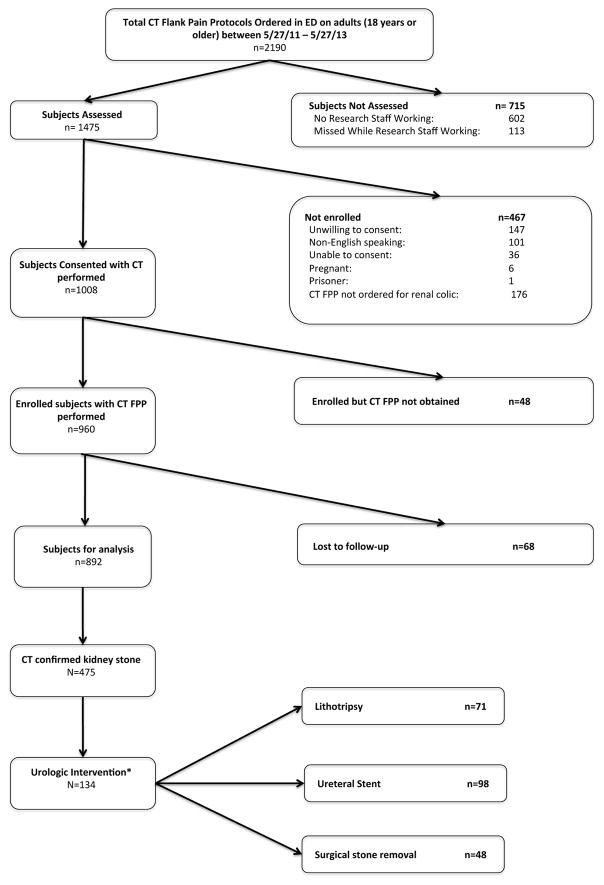
This secondary analysis of prospective data included patients with an obstructing ureteral stone that was confirmed by computerized tomography in an emergency department. All patients also underwent point of care limited renal ultrasound. The need for urological intervention at 90 days was assessed by a followup interview. Logistic regression was used to identify predictors of admission and urological intervention, which were further stratified by disposition. Separate regression models with and without computerized tomography findings (point of care limited renal ultrasound only) were compared using c-statistics.
Among a cohort of 475 patients with a symptomatic stone on computerized tomography 95 (20%) were admitted and 68 (72%) received an intervention. Of 380 discharged patients 66 (17%) required urological intervention. Admitted patients were more likely to have undergone a prior procedure, have evidence of kidney injury or infection, need opiate analgesia or have larger stones or hydronephrosis on point of care limited renal ultrasound. Predictors of intervention varied by disposition. However, regression models with and without computerized tomography findings demonstrated similar c-statistics. Discharged patients with larger stones, a longer pain duration at presentation and prior procedures were more likely to undergo intervention.
Intervention was common among admitted patients but it occurred in a minority of those discharged. Predictors of intervention varied by disposition. Models incorporating computerized tomography findings were similar to those that did not incorporate such findings. These data support ultrasound first or delayed computerized tomography diagnostic pathways for patients deemed clinically suitable for discharge home.
每年有超过 100 万名患者因肾结石到急诊科就诊,但只有少数患者需要住院治疗或接受泌尿科手术。我们描述了住院或泌尿科干预的预测因素。
这项前瞻性数据的二次分析包括在急诊科通过计算机断层扫描(CT)确诊为输尿管梗阻性结石的患者。所有患者还接受了即时有限肾脏超声检查。通过随访访谈评估 90 天时是否需要泌尿科干预。使用逻辑回归确定住院和泌尿科干预的预测因素,并按处置进行分层。使用 C 统计量比较了有和没有 CT 结果(仅即时有限肾脏超声)的回归模型。
在 CT 上有症状结石的 475 例队列中,有 95 例(20%)住院,68 例(72%)接受了干预。在 380 例出院患者中,有 66 例(17%)需要泌尿科干预。住院患者更有可能接受过先前的手术,有肾脏损伤或感染的证据,需要阿片类镇痛药,或在即时有限肾脏超声上有更大的结石或肾积水。干预的预测因素因处置方式而异。然而,有和没有 CT 结果的回归模型表现出相似的 C 统计量。在即时有限肾脏超声上有较大结石、就诊时疼痛持续时间较长和有先前手术史的出院患者更有可能接受干预。
住院患者中干预很常见,但在出院患者中仅占少数。干预的预测因素因处置方式而异。纳入 CT 结果的模型与不纳入此类结果的模型相似。这些数据支持对认为适合出院回家的患者进行超声优先或延迟 CT 诊断途径。