Department of Critical Care Medicine, Guangdong General Hospital, Guangdong Academy of Medical Sciences, Guangzhou, 510080, Guangdong Province, P.R. China.
Department of Critical Care Medicine, Xiaolan Hospital of Southern Medical University, Zhongshan, 528415, Guangdong, P.R. China.
Sci Rep. 2017 Jun 26;7(1):4245. doi: 10.1038/s41598-017-04627-3.
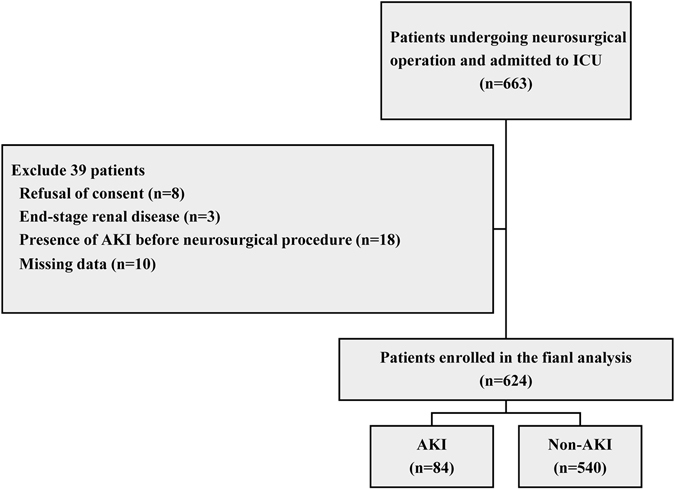
We investigated the incidence, perioperative risk factors, and outcomes of postoperative acute kidney injury (AKI) in neurosurgical critically ill patients. A prospective multicenter cohort study was conducted, enrolling adult patients who underwent neurosurgical procedure and admitted to the neurosurgical intensive care units (ICU). Postoperative AKI was diagnosed within 7 days after surgery based on the Kidney Disease Improving Global Outcomes criteria. Of 624 enrolled patients, postoperative AKI occurred in 84 patients. AKI was associated with increased rates of ICU and in-hospital mortality, postoperative renal replacement therapy, postoperative tracheotomy, and postoperative tracheal reintubation. Patients who developed AKI had higher total ICU costs, prolonged length of hospital and ICU stay, and longer duration of postoperative mechanical ventilation. Multivariate analysis identified postoperative reoperation (adjusted odds ratio [OR] 5.70 [95% CI, 1.61-20.14]), postoperative concentration of serum cystatin C (adjusted OR 4.53 [95% CI, 1.98-10.39]), use of mannitol during operation (adjusted OR 1.97 [95% CI, 1.13-3.43]), postoperative APACHE II score (adjusted OR 1.11 [95% CI, 1.06-1.16]), and intraoperative estimated blood loss (adjusted OR 1.04 [95% CI, 1.00-1.08]) as independent risk factors for postoperative AKI. Postoperative AKI in neurosurgical critically ill cohort is prevalent and associated with adverse in-hospital outcomes.
我们研究了神经外科危重症患者术后急性肾损伤(AKI)的发生率、围手术期危险因素和结局。进行了一项前瞻性多中心队列研究,纳入了接受神经外科手术并入住神经外科重症监护病房(ICU)的成年患者。术后 AKI 根据肾脏病改善全球结局标准在术后 7 天内诊断。在纳入的 624 名患者中,84 名患者发生术后 AKI。AKI 与 ICU 和住院死亡率增加、术后肾脏替代治疗、术后气管切开术和术后气管再插管相关。发生 AKI 的患者 ICU 总费用更高,住院和 ICU 住院时间延长,术后机械通气时间延长。多变量分析确定了术后再次手术(调整后的优势比 [OR] 5.70 [95% CI,1.61-20.14])、术后血清胱抑素 C 浓度(调整后的 OR 4.53 [95% CI,1.98-10.39])、手术期间使用甘露醇(调整后的 OR 1.97 [95% CI,1.13-3.43])、术后急性生理与慢性健康评分 II (调整后的 OR 1.11 [95% CI,1.06-1.16])和术中估计失血量(调整后的 OR 1.04 [95% CI,1.00-1.08])是术后 AKI 的独立危险因素。神经外科危重症患者术后 AKI 很常见,与不良住院结局相关。