Matignon Marie, Pilon Caroline, Commereuc Morgane, Grondin Cynthia, Leibler Claire, Kofman Tomek, Audard Vincent, Cohen José, Canoui-Poitrine Florence, Grimbert Philippe
AP-HP, Henri Mondor Hospital, Nephrology and Transplantation Department and CIC Biothérapies 504, Créteil, France.
INSERM U955, Team 21, Créteil, France and Paris Est University (UPEC), Créteil, France.
PLoS One. 2017 Jun 27;12(6):e0178572. doi: 10.1371/journal.pone.0178572. eCollection 2017.
Approximately 25% of kidney transplant recipients develop de novo anti-HLA donor-specific antibodies (dnDSA) leading to acute antibody-mediated rejection (ABMR) in 30% of patients. Preemptive therapeutic strategies are not available.
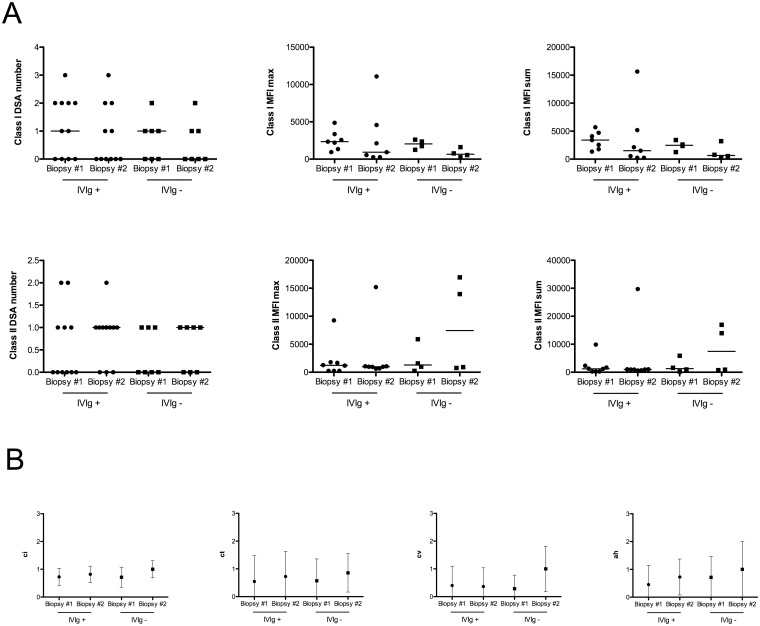
We conducted a prospective observational study including 11 kidney transplant recipients. Inclusion criteria were dnDSA occurring within the first year after transplant and normal allograft biopsy. All patients were treated with high-dose IVIG (2 g/kg 0, 1 and 2 months post-dnDSA). The primary efficacy outcome was incidence of clinical and subclinical acute ABMR within 12 months after dnDSA detection as compared to a historical control group (IVIG-).
Acute ABMR occurred in 2 or 11 patients in the IVIG+ group and in 1 of 9 patients in the IVIG- group. IVIG treatment did not affect either class I or class II DSA, as observed at the end of the follow-up. IVIG treatment significantly decreased FcγRIIA mRNA expression in circulating leukocytes, but did not affect the expression of any other markers of B cell activation.
In this first pilot study including kidney allograft recipients with early dnDSA, preemptive treatment with high-dose IVIG alone did not prevent acute ABMR and had minimal effects on DSA outcome and B cell phenotype.
约25%的肾移植受者会产生新发抗人白细胞抗原(HLA)供体特异性抗体(dnDSA),其中30%的患者会发生急性抗体介导的排斥反应(ABMR)。目前尚无抢先治疗策略。
我们开展了一项前瞻性观察性研究,纳入了11例肾移植受者。纳入标准为移植后第一年内出现dnDSA且移植肾活检结果正常。所有患者均接受大剂量静脉注射免疫球蛋白(IVIG)治疗(dnDSA检测后0、1和2个月时给予2 g/kg)。主要疗效指标是与历史对照组(未接受IVIG治疗组)相比,dnDSA检测后12个月内临床和亚临床急性ABMR的发生率。
IVIG治疗组11例患者中有2例发生急性ABMR,未接受IVIG治疗组9例患者中有1例发生急性ABMR。随访结束时观察发现,IVIG治疗对I类或II类DSA均无影响。IVIG治疗可显著降低循环白细胞中FcγRIIA mRNA的表达,但不影响B细胞活化的任何其他标志物的表达。
在这项纳入早期dnDSA的肾移植受者的初步试验研究中,单独使用大剂量IVIG进行抢先治疗并不能预防急性ABMR,且对DSA结果和B细胞表型的影响极小。