Colafrancesco Serena, Priori Roberta, Valesini Guido, Argolini Lorenza, Baldissera Elena, Bartoloni Elena, Cammelli Daniele, Canestrari Giovanni, Cantarini Luca, Cavallaro Elena, Cavalli Giulio, Cerrito Lucia, Cipriani Paola, Dagna Lorenzo, Marchi Ginevra De, Vita Salvatore De, Emmi Giacomo, Ferraccioli Gianfranco, Frassi Micol, Galeazzi Mauro, Gerli Roberto, Giacomelli Roberto, Gremese Elisa, Iannone Florenzo, Lapadula Giovanni, Lopalco Giuseppe, Manna Raffaele, Mathieu Alessandro, Montecucco Carlomaurizio, Mosca Marta, Piazza Ilaria, Piga Matteo, Pontikaki Irene, Romano Micol, Rossi Silvia, Rossini Maurizio, Ruscitti Piero, Silvestri Elena, Stagnaro Chiara, Talarico Rosaria, Tincani Angela, Viapiana Ombretta, Vitiello Gianfranco, Fabris Francesca, Bindoli Sara, Punzi Leonardo, Galozzi Paola, Sfriso Paolo
Rheumatology Unit, Department of Internal Medicine and Medical Specialties, Sapienza University of RomeRome, Italy.
Division of Rheumatology, ASST Gaetano PiniMilan, Italy.
Front Pharmacol. 2017 Jun 13;8:369. doi: 10.3389/fphar.2017.00369. eCollection 2017.
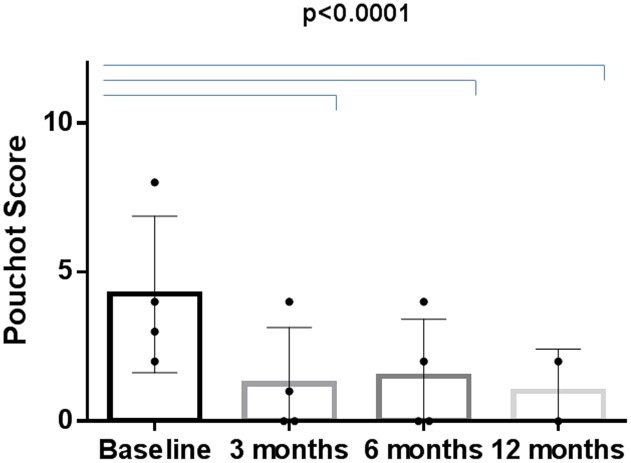
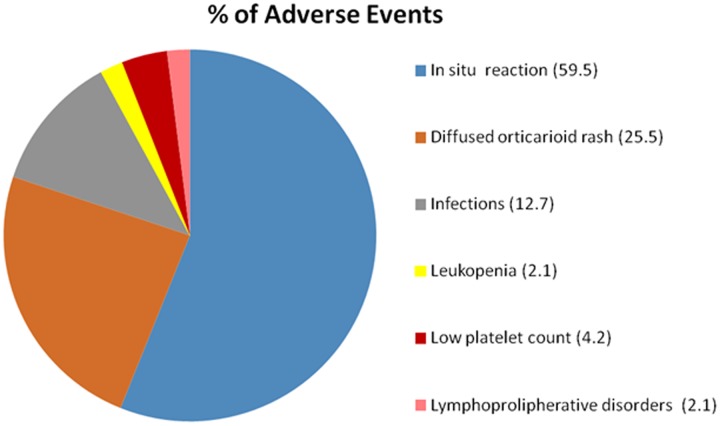
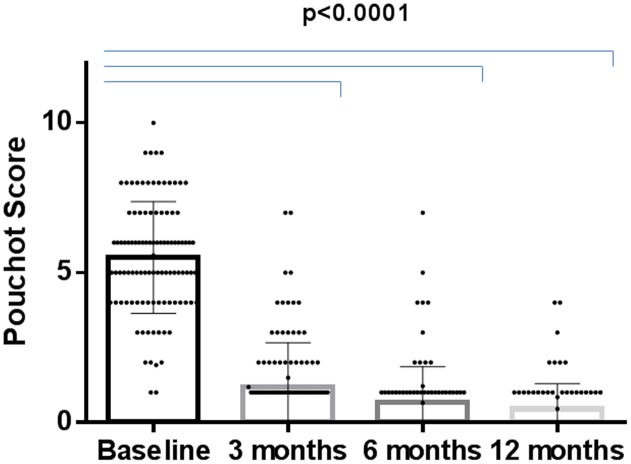
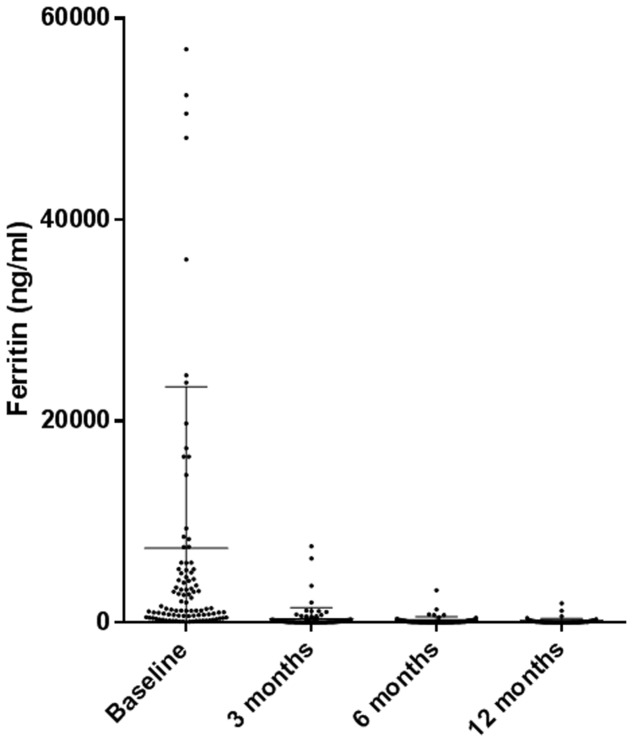
Interleukin (IL)-1 plays a crucial role in the pathogenesis of Adult onset Still's disease (AOSD). To evaluate the efficacy and safety of anakinra (ANA) and canakinumab (CAN) in a large group of AOSD patients. Data on clinical, serological features, and concomitant treatments were retrospectively collected at baseline and after 3, 6, and 12 months from AOSD patients (Yamaguchi criteria) referred by 18 Italian centers. Pouchot's score was used to evaluate disease severity. One hundred forty patients were treated with ANA; 4 were subsequently switched to CAN after ANA failure. The systemic pattern of AOSD was identified in 104 (74.2%) of the ANA-treated and in 3 (75%) of the CAN-treated groups; the chronic-articular type of AOSD was identified in 48 (25.8%) of the ANA-treated and in 1 (25%) of the CAN-treated groups. Methotrexate (MTX) was the most frequent disease modifying anti-rheumatic drug (DMARD) used before beginning ANA or CAN [91/140 (75.8%), 2/4 (50%), respectively]. As a second-line biologic DMARD therapy in 29/140 (20.7%) of the patients, ANA was found effective in improving all clinical and serological manifestations ( < 0.0001), and Pouchot's score was found to be significantly reduced at all time points ( < 0.0001). No differences in treatment response were identified in the ANA-group when the patients were stratified according to age, sex, disease pattern or mono/combination therapy profile. ANA primary and secondary inefficacy at the 12-month time point was 15/140 (10.7%) and 11/140 (7.8%), respectively. Adverse events (AEs) [mainly represented by in situ (28/47, 59.5%) or diffuse (12/47, 25.5%) skin reactions and infections (7/47, 14.8%)] were the main causes for discontinuation. Pouchot's score and clinical and serological features were significantly ameliorated at all time points ( < 0.0001) in the CAN-group, and no AEs were registered during CAN therapy. Treatment was suspended for loss of efficacy only in one case (1/4, 25%). This is the largest retrospective observational study evaluating the efficacy and safety of IL-1 inhibitors in AOSD patients. A good response was noted at 3 months after therapy onset in both the ANA- and CAN-groups. Skin reaction may nevertheless represent a non-negligible AE during ANA treatment.
白细胞介素(IL)-1在成人斯蒂尔病(AOSD)的发病机制中起关键作用。为评估阿那白滞素(ANA)和卡那单抗(CAN)在一大群AOSD患者中的疗效和安全性。回顾性收集了18个意大利中心转诊的AOSD患者(符合山口标准)在基线以及3、6和12个月后的临床、血清学特征及伴随治疗的数据。采用Pouchot评分评估疾病严重程度。140例患者接受ANA治疗;其中4例在ANA治疗失败后改用CAN。ANA治疗组中104例(74.2%)和CAN治疗组中3例(75%)为AOSD全身型;ANA治疗组中48例(25.8%)和CAN治疗组中1例(25%)为AOSD慢性关节型。甲氨蝶呤(MTX)是开始ANA或CAN治疗前最常用的改善病情抗风湿药物(DMARD)[分别为91/140(75.8%),2/4(50%)]。在29/140(20.7%)的患者中,ANA作为二线生物DMARD治疗,被发现可有效改善所有临床和血清学表现(<0.0001),且在所有时间点Pouchot评分均显著降低(<0.0001)。根据年龄、性别、疾病类型或单药/联合治疗情况对ANA组患者进行分层时,未发现治疗反应存在差异。ANA在12个月时的原发性和继发性无效分别为15/140(10.7%)和11/140(7.8%)。不良事件(AE)[主要表现为局部(28/47,59.5%)或弥漫性(1十二条/47,25.5%)皮肤反应和感染(7/47,14.8%)]是停药的主要原因。CAN组在所有时间点Pouchot评分以及临床和血清学特征均显著改善(<0.0001),且CAN治疗期间未记录到AE。仅1例(1/4,25%)因疗效丧失而暂停治疗。这是评估IL-1抑制剂在AOSD患者中疗效和安全性的最大规模回顾性观察研究。ANA组和CAN组在治疗开始后3个月均观察到良好反应。然而,皮肤反应可能是ANA治疗期间不可忽视的AE。